Downloaded 97 times



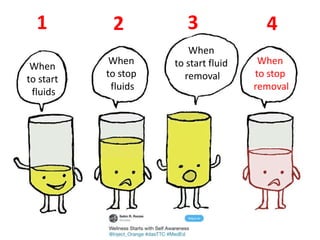
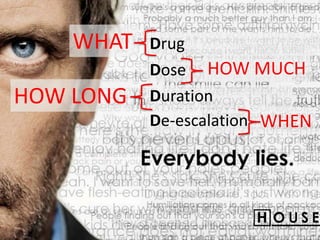


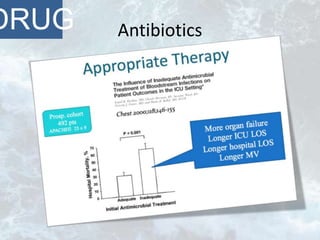




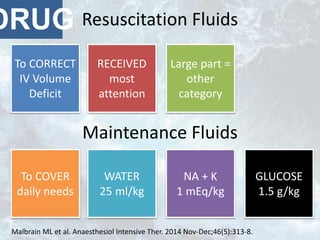




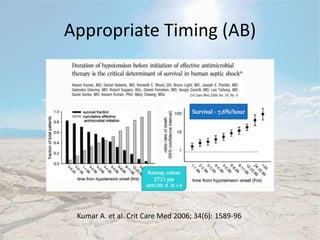
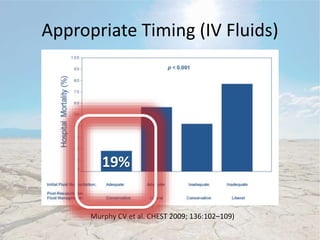

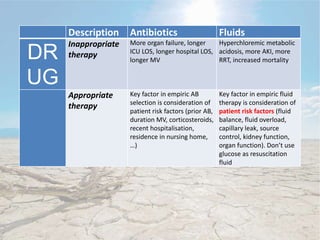
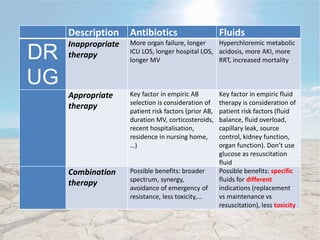
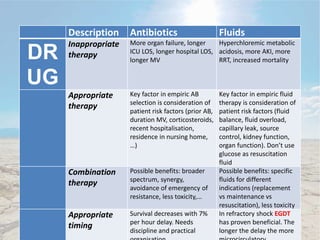

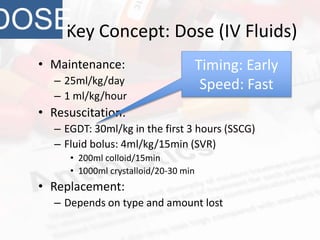
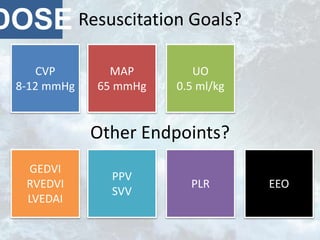
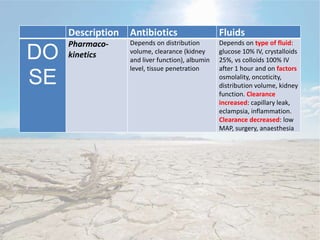
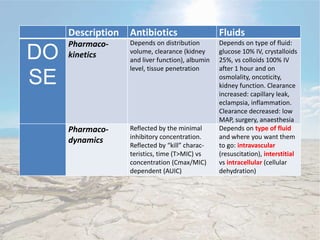
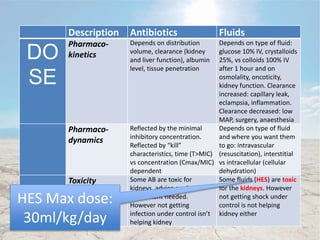

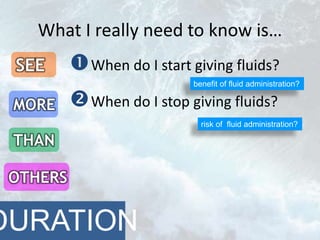

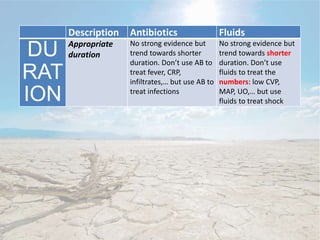
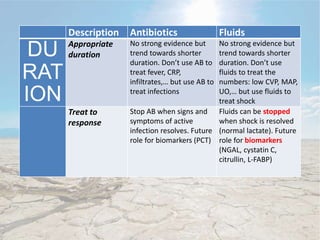


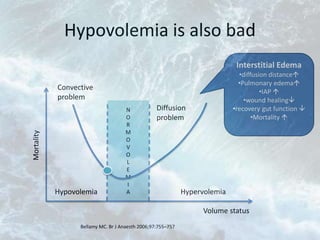

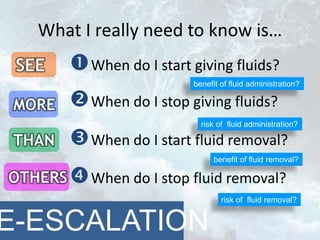
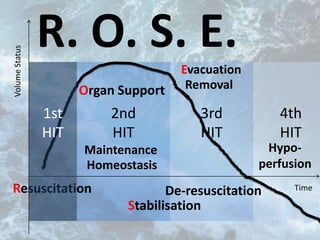
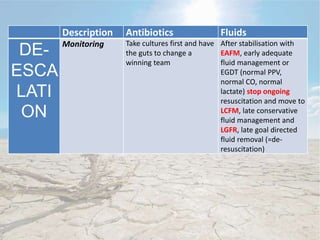







This document discusses fluid management in intensive care patients. It notes that fluids are drugs that require appropriate dosing, timing, and de-escalation. Inappropriate fluid therapy can lead to hyperchloremic metabolic acidosis, acute kidney injury, and increased mortality. The key factors in empiric fluid therapy are considering patient risk factors for fluid overload and targeting fluids specifically for resuscitation, maintenance, or replacement needs rather than focusing solely on hemodynamic parameters. Fluid removal should begin when shock is resolved to avoid complications from fluid overload.























































































