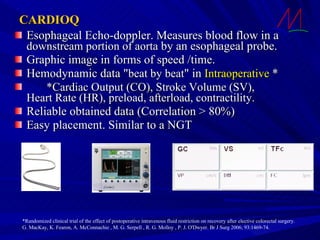
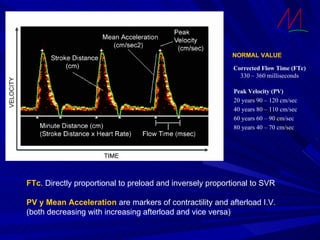
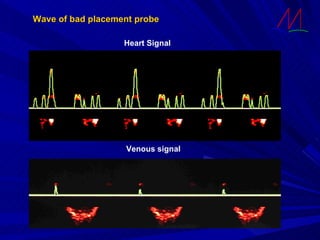
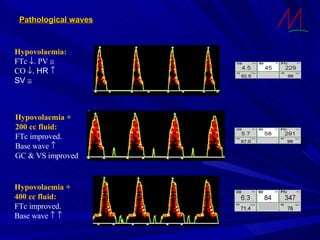
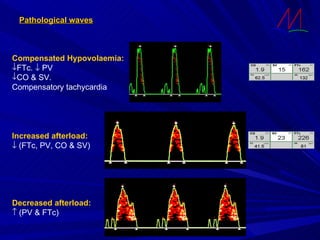
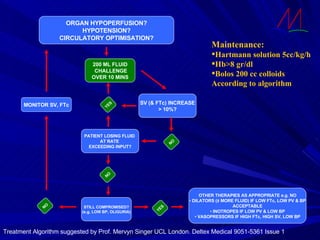
The document discusses the use of esophageal echo-doppler (EED) in fast-track surgery and fluid management. EED can non-invasively measure cardiac output andpreload, helping optimize fluid therapy. It provides hemodynamic data beat-to-beat during surgery. EED values like corrected flow time and peak velocity indicate fluid responsiveness and contractility. The data aid clinical decisions on fluid boluses or vasoactive drugs to ensure adequate perfusion and reduce morbidity. However, EED has limitations like aortic geometry assumptions and signal disruption from ventilation or probes.




























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





