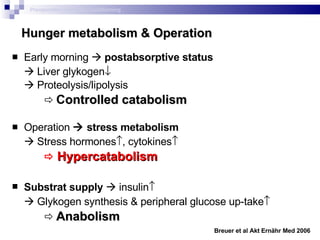
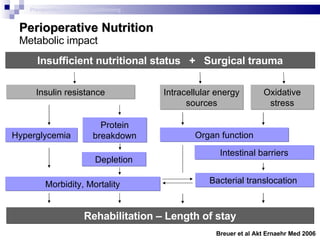
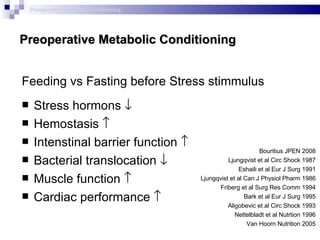
The document discusses preoperative metabolic conditioning and fasting guidelines. It summarizes several studies that show:
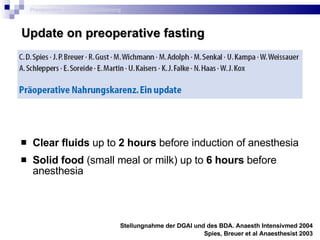
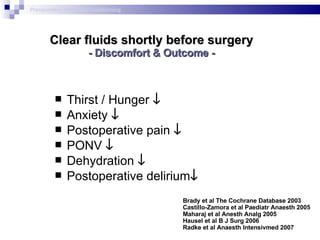
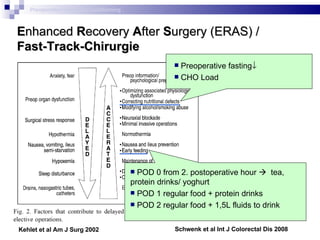
1) Clear fluids can be consumed up to 2 hours before surgery and solid foods up to 6 hours with no increased risk of complications.
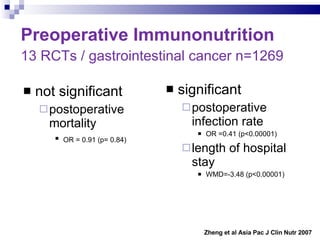
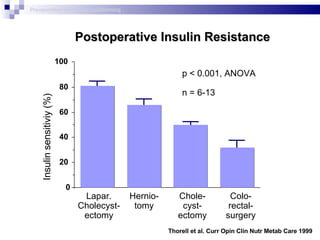
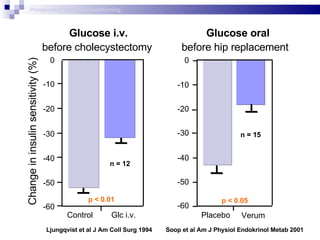
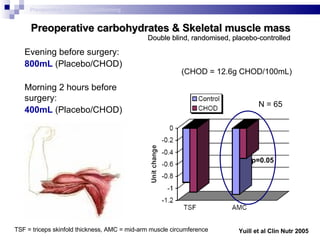
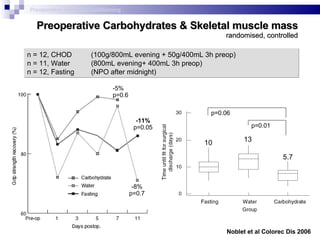
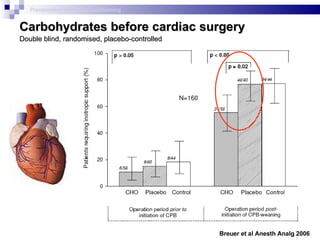
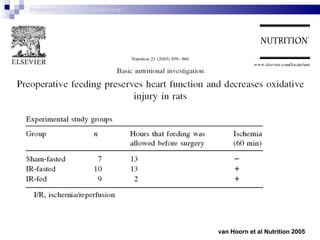
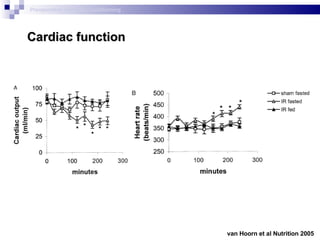
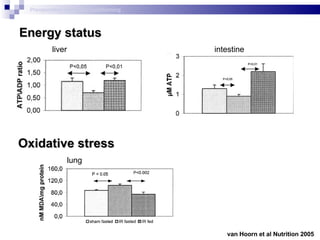
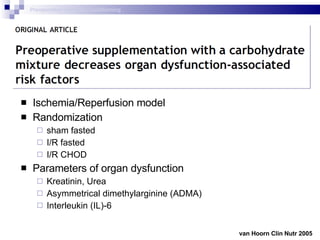
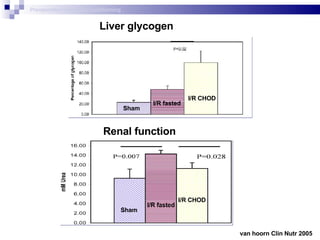
2) Preoperative carbohydrate loading improves postoperative insulin sensitivity, muscle mass, and cardiac and organ function compared to fasting.
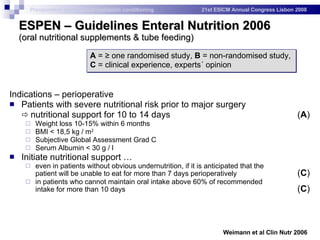
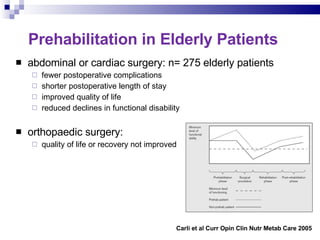
3) Preoperative nutritional support is recommended for patients with severe pre-existing nutritional risk or those requiring prolonged postoperative fasting.
![Cochrane-Analysis 38 randomized controlled comparisons (22 trials) Objects: perioperative complications & comfort “ […] no evidence to suggest a shortened fluid fast results in an increased risk of aspiration or related morbidity […].” Level of Evidence = 1a “ […] appraise this evidence for themselves and […] adjust any remaining standard fasting policies for patients that are not considered `at risk´ during anaesthesia.” Grade of Recommendation = A Brady et al The Cochrane Collaboration 2003 Preoperative metabolic conditioning](https://image.slidesharecdn.com/preoperativemetabolicconditioning-090508091651-phpapp01/85/Preoperative-Metabolic-Conditioning-6-320.jpg)
![„ From the metabolic and nutritional point of view, the key aspects of perioperative care include: avoidance of long periods of pre-operative fasting; re-establishment of oral feeding as early as possible after surgery; integration of nutrition into the overall management of the patient; […]“ Weimann et al Clin Nutr 2006](https://image.slidesharecdn.com/preoperativemetabolicconditioning-090508091651-phpapp01/85/Preoperative-Metabolic-Conditioning-22-320.jpg)