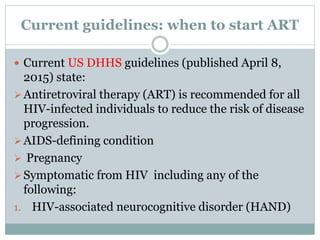
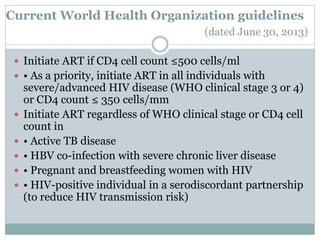
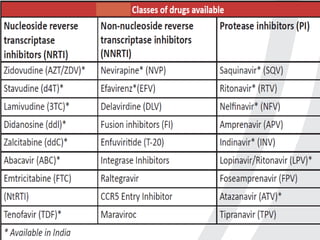
Highly Active Antiretroviral Therapy (HAART) involves using a combination of at least three antiretroviral drugs to suppress the HIV virus and stop the progression of HIV disease. HAART decreases the viral load, improves immune function, and prevents opportunistic infections. The goals of HAART are to prolong life, improve quality of life, maximize viral suppression, and reconstitute the immune system. Current guidelines recommend starting HAART for all HIV patients regardless of CD4 count. Proper counseling, adherence, monitoring, and management of side effects are important for the success of HAART.