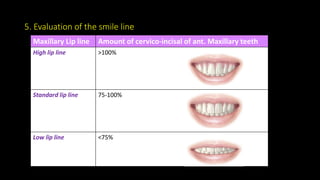
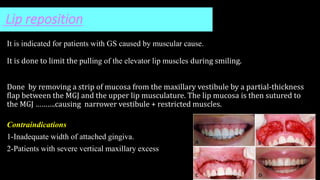
The document provides an extensive overview of gummy smile, detailing its etiology, diagnosis, and various treatment modalities including surgical and non-surgical options. It discusses causes such as periodontal deformities and soft tissue issues, and presents evaluation methods for identifying gummy smile, along with measurements for facial and dental proportions. Treatment options range from orthodontic and restorative approaches to specific surgical interventions like crown lengthening and myectomy.

















































































![gummy smile ... by sampita dhali (1) [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/gummysmile-240822170221-bbfd4416-thumbnail.jpg?width=640&height=640&fit=bounds)











































