The document discusses several topics related to facial growth and development:
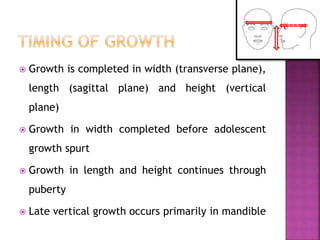
- Facial growth is completed in width, length, and height, with growth in width finishing before puberty and growth in length and height continuing through puberty.
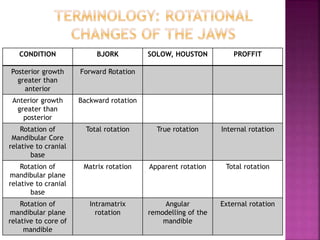
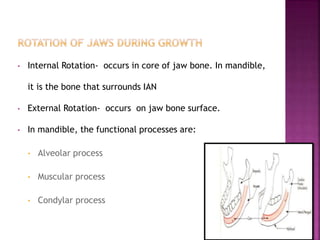
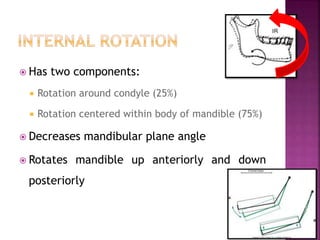
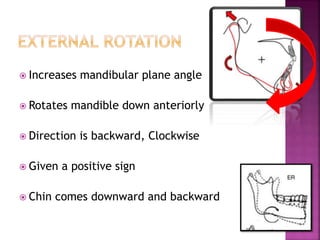
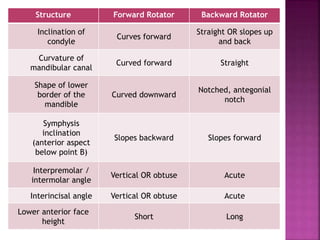
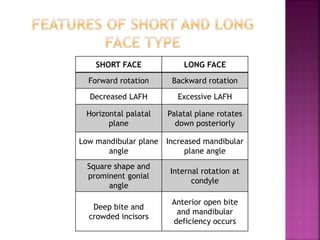
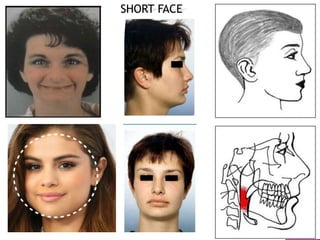
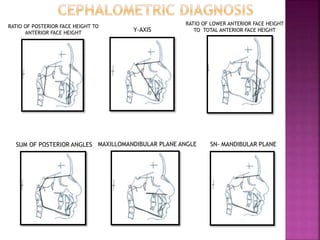
- The mandible can undergo internal and external rotation, affecting the mandibular plane angle and position of the chin.
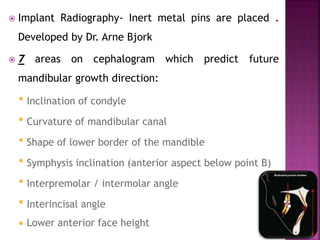
- Factors like inclination of the condyle can predict whether future mandibular growth will involve forward or backward rotation.
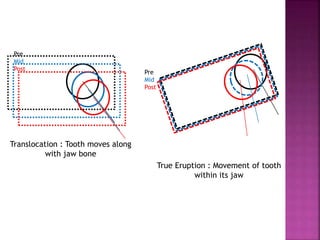
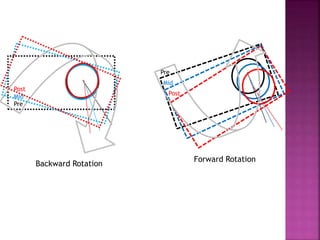
- Jaw rotation influences tooth eruption and positioning, with forward rotation tipping incisors forward and backward rotation uprighting them.