
Recommended
More Related Content
Similar to Guillain-Barre Syndrome Transmissional respiratory and gastrointestinal diagram .pdf
Similar to Guillain-Barre Syndrome Transmissional respiratory and gastrointestinal diagram .pdf (20)
Recently uploaded
Recently uploaded (20)
Guillain-Barre Syndrome Transmissional respiratory and gastrointestinal diagram .pdf
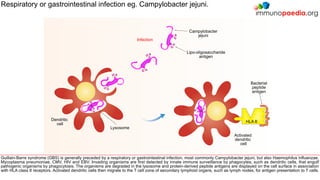
- 1. Guillain-Barre syndrome (GBS) is generally preceded by a respiratory or gastrointestinal infection, most commonly Campylobacter jejuni, but also Haemophilus influenzae, Mycoplasma pneumoniae, CMV, HIV and EBV. Invading organisms are first detected by innate immune surveillance by phagocytes, such as dendritic cells, that engulf pathogenic organisms by phagocytosis. The organisms are degraded in the lysosome and protein-derived peptide antigens are displayed on the cell surface in association with HLA class II receptors. Activated dendritic cells then migrate to the T cell zone of secondary lymphoid organs, such as lymph nodes, for antigen presentation to T cells. Campylobacter jejuni Infection HLA II Respiratory or gastrointestinal infection eg. Campylobacter jejuni. Dendritic cell Bacterial peptide antigen Lysosome Activated dendritic cell Lipo-oligosaccharide antigen
- 2. Activated dendritic cells present protein-derived peptide antigens to CD4+ helper T cells in the T cell zone of secondary lymphoid organs, such as lymph nodes. Recognition of peptide antigens by the T cell receptor (TCR) activates CD4+ T cells and induces cell proliferation which generates antigen-specific effector and memory T cells. Although T-independent mechanisms for activating B cells are known, interaction with helper T cells is usually needed to allow B cells to differentiate into plasma cells and to switch from IgM to other antibody isotypes, such as IgG, as well as to induce affinity maturation of antibodies and memory cell differentiation. In GBS, cross-reactive antibodies are class-switched suggesting a role for helper T cells. Naive CD4+ Helper T Lymphocyte CD4 TCR Antigen-specific CD4+ helper T lymphocyte activation. Activated CD4+ Helper T Lymphocyte TCR CD4 HLA II Bacterial peptide antigen Secondary lymphoid organ T cell zone Activated dendritic cell
- 3. In GBS, it is thought that antibodies initially directed towards lipo-oligosaccharide antigens later cross-react with similar epitopes (molecular mimicry), such as gangliosides found on neurons or myelin. These antibodies are produced by B cells primed and activated in the secondary lymphoid organs where lipo-oligosaccharide antigens are displayed on the surface of follicular dendritic cells. Naive B cells expressing B cell receptors (BCR) that recognise these antigens induce endocytosis of the antigen-receptor complex. Although the antigen targeted by the antibody is not a protein, it is likely that pathogen-derived proteins are involved in B cell activation since recruitment of T cell help is needed to induce isotype-switched antibodies seen in GBS. “Naive” B Lymphocyte Antigen-specific B lymphocyte priming Lipo-oligosaccharide antigen B cell receptor (BCR) HLA II “Primed” B Lymphocyte Campylobacter jejuni Secondary lymphoid organ B cell zone Follicular dendritic cell Germinal centre ? Unknown bacterial peptide epitope
- 4. Primed B cells display peptide antigens bound to HLA class II receptors and become activated by previously activated CD4+ helper T cells that recognise specific peptide antigen via the TCR. The BCR is targeted to lipo-oligosaccharide antigens which do not bind to HLA class II receptors, therefore it is likely that a peptide antigen, which is unknown in GBS, is presented to T cells in order activate B cells and permit isotype switching. Although T-independent mechanisms for producing IgG2 antibodies in response to polysaccharide antigens are known, in GBS, cross-reactive antibodies are of the IgG1 and IgG3 subclass which are T-dependent, potent activators of the classical complement cascade and bind strongly to Fc receptors on phagocytes, such as macrophages. Antigen-specific B lymphocyte activation Plasma B cell Isotype switched IgG1 or IgG3 Secondary lymphoid organ T cell zone Activated CD4+ Helper T Lymphocyte Activated B Lymphocyte CD4 HLA II ? Unknown bacterial peptide antigen TCR
- 5. Clearance of invading organisms is mediated by soluble antibodies of the IgM and IgG class that bind to the surface of the pathogen and tag them for destruction by effector mechanisms of the innate immune system. These include classical complement activation (IgG and IgM) and formation of the membrane attack complex, antibody-dependent cell cytotoxicity (ADCC) mediated by Fc receptors on natural killer cells (IgG) and receptor-mediated phagocytosis via opsonisation of the pathogen with IgG or complement C3b proteins, mediated by Fc receptors and complement receptors on phagocytes. In GBS, however, cross-reactive IgG antibodies will begin to trigger similar immune attacks against peripheral nerves. IgG IgM Campylobacter jejuni Antibody dependent cell cytotoxicty (ADCC) Natural killer cell Antibody-mediated destruction of the pathogen Classical complement pathway Receptor- mediated phagocytosis C3b Anti- lipo-oligosaccharide antibodies Macrophage Complement receptor Fc receptor C1
- 6. The most common subtype of GBS is demyelination associated with infiltration of macrophages and CD4+ helper T cells into peripheral nerve tissue (usually sensory or motor neurons). It is thought that anti-myelin IgG antibodies mediate destruction of myelin via activation of the classical complement cascade and formation of the membrane attack complex as well as activation of macrophages expressing Fc receptors and complement receptors that faciliate stripping of myelin. Further enhancement of macrophage activity may be provided by infiltration of activated CD4+ helper T cells that secrete pro-inflammatory cytokines, such as IFN-γ and TNF-α. Muscle fibres Neuron Demyelination of nerve cells. Myelin antigen Myelin sheath C1 C3b CD4+ helper T lymphocyte Motor- nerve end-plate terminal Membrane attack complex IFN-γ TNF-α. anti- myelin IgG Blood-nerve barrier C5b-9 Macrophage Fc receptor Complement receptor Receptor- mediated phagocytosis
- 7. A less common subtype of GBS involves immunological damage to the axon or motor-nerve end-plate terminals and is mediated by anti-ganglioside IgG antibodies. The symptoms and severity depend on the type of ganglioside targeted since the membrane distribution of these molecules on nerve cells varies. Similar so demyelinating GBS, nerve damage is caused by activation of the classical complement cascade and formation of the membrane attack complex or by infiltration of macrophages expressing Fc receptors for IgG or complement receptors for complement C3b that initiate destructive phagocytic processes. Neuron Axonal or end-plate terminal damage. Ganglioside Myelin sheath C1 C3b Nerve axon Muscle fibres Membrane attack complex Motor- nerve end-plate terminal anti- ganglioside IgG Blood-nerve barrier C5b-9 Macrophage Fc receptor Complement receptor Receptor- mediated phagocytosis