Downloaded 16 times
![Start by putting the patient at ease: ( )
• Greet the patient by name: "Good morning, Mrs Jones"
• Introduce yourself and explain that you are a medical student.
• Shake the patient's hand, or if they are unwell rest your hand on theirs.
• Ensure that the patient is comfortable.
You should always begin the physician-centered phase of the interview with "WH"
questions (where? what? when?) directed at the chief complaint(s). Build on the
information the patient has already given you. Flesh out areas of the story you don't
fully understand. Try to quantify whenever possible (pain on a scale of 1 to 10,
number of days instead of "a while," etc.). Be as specific as possible and try to record
what the patient says accurately, without interpretation
A.Personal history:
1- Name:
Medical registration
To be familiar with patient
2-Age: Why we ask about age: "age related diseases as:
"
Infant (0-2 yrs) --- congenital diseases
Childhood (2-12 yrs) --- Parasitic infection mumps
Adolescence (12-20 yrs) --- Trauma, TB
Adulthood (20-40yrs)--- Hernia )
Middle age (40-60yrs) --- Gall bladder diseases, Atherosclerosis
Old age (above 60rs --) --- Malignancy, vascular disease)
3. Sex: Why sex: "sex related diseases"
emale
Breast cancer
Gall bladder stones
Femoral Hernia
Goiter
SLE "Systemic Lupus Erythematosis"
ale
Hypertension
Inguinal hernia
Peptic ulcer
Gastric and bladder carcinoma
4- Residence: íÚ^Î÷]<á^ÓÚ
Farmer ---- Malnutrition and parasitic infection "bilharziasis"
Endemic diseases: Oases ---goitre
Bilharziasis---Egypt
stomach cancer Japan
Burkett's lymphoma central Africa, esophageal cancer china
1](https://image.slidesharecdn.com/gsur302-120518151143-phpapp02/85/Gsur-302-2-320.jpg)


![1. Onset:
o Sudden "trauma hematoma" _MCQ_
o Gradual "neoplasia"
o Acute "inflammation, infection"
o Accidental "discovered by patient or others"
2. Course:
o Progressive rapid "malignant lesion" or slow
"Benign lesion"
o Regressive acute infection
o Stationary cysts or benign lesion
o Intermittent jaundice due to obstruction
3. Duration:
o Short "inflammation
o Long "benign lesion"
4. Relation to pain:
o Swelling then pain --malignancy
o Pain then swelling- inflammation
5. Relation of onset to constitutional manifestation:
o Fever , redness, headache, malaise
6. effect on body function and nearby structures
7. possible cause (aetiology):
o Carrying Heavy object -- hernia
o Trauma -› hematoma
8. Special character:
o Move up and down with deglutition thyroid swelling
o increase size with food pharyngeal diverticulum
o Pulsations aneurysms or vascular swelling
o Impulse on cough and reduce on laying down hernia
D.past history:
ê•^¹]<<»<˜è†¹]<äe^‘]<‚Î<^Ú<<àÂ<Ù^ŠÞ<
The past medical history is essentially background information related to the
patient's health and well being. A brief past medical (and social) history often
includes these elements
General question:
• Have you suffered from any previous illness?
1. Allergies and Reactions to Drugs (What happened?)
2. Current Medications (Including "Over-the-Counter")
3. Medical/Psychiatric Illnesses (Diabetes, Hypertension, Depression, etc.)
4. Surgeries/Injuries/Hospitalizations (Appendectomy, Car Accident, etc.)
5. Immunizations
6. smocking/Alcohol
4](https://image.slidesharecdn.com/gsur302-120518151143-phpapp02/85/Gsur-302-5-320.jpg)


![B) palpation ‚éÖ^e<Œ^Šu÷]<
1-tenderness اﻻﻟﻢ ﻋﻨﺪ اﻟﻠﻤﺲ
2-Temperature- by dorsum of hand which is more dry
3-consistency :
solid :
• Hard like bone
• Firm like tip of nose
• Soft like lobule of ear
Systic : fluctuant "presences of fluid" (MCQ )
Can be detected by:
• fluctuation test : -
- cross fluctuation test
- Bipolar fluctuation test- for swelling have 2 place
NB . fluctuation test uses > 2 cm
Pagets test uses < 2 cm
4-Edge:
well defined edges or ill defined edges
remember . comment on edge by palpation ( MCQ )
C) Percussion:
• Resonant: gaseous swellings
• Dull: cyst and solid swellings
D) Auscultation:
• Systolic murmurs in aneurysm
• Contentious murmurs in A/V fistula
• Venous hum in portal hypertention
• Intestinal sounds in hernias
7](https://image.slidesharecdn.com/gsur302-120518151143-phpapp02/85/Gsur-302-8-320.jpg)


![complication of suturing a wound
1- infection :
♦ tools not clean
♦ disease transmission (as AIDS)
♦ inflammation ( auto immune Reaction)
2- scar
♦ wound healing but leave mark
♦ not raised / not elevated
♦ respect edges of wound
3- , keloid (occur more with natural)
♦ spread out of wound edges
♦ itching
♦ raised
4- improper healing (opened the wound)
BN .(radiotherapy) : ( endarteitis obliteranis )
i.e small vessels are blocked lead to impair healing
BN . Human glue ( skin stripsskin dips)
@ @ZÛíjïÑÜa@ôÝÈ@bäíØŠb’
< <†’Ú<íÃÚ^q<»<|^rßÖ]<Ðè†ŞÖ<Ôu^jËÚ
<www.facebook.com/dr.alshamali
< <ÜÓñ^Â<gé<àÚ<^ÞçŠßi÷
10](https://image.slidesharecdn.com/gsur302-120518151143-phpapp02/85/Gsur-302-11-320.jpg)

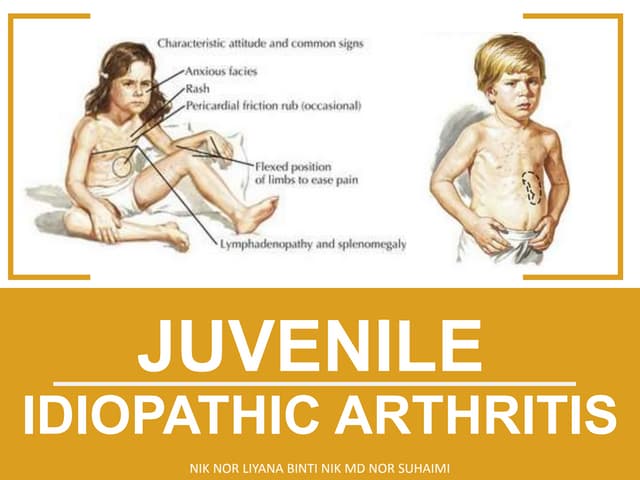
1. This document provides guidance on performing a patient examination, including taking a medical history and conducting a physical examination of a swelling. 2. It details the key components of a patient's medical history to cover, such as their personal history, present complaint, past medical history, and family history. 3. The document also describes how to physically examine a swelling, including inspecting it, palpating it, performing percussion and auscultation, and discussing different types of sutures used in surgery.