Download as PDF, PPTX





















































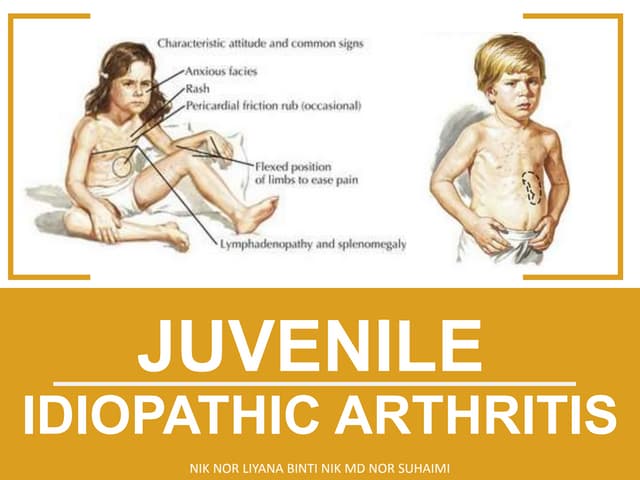
The document discusses juvenile idiopathic arthritis (JIA), the most common pediatric rheumatologic disease, outlining its definitions, classification, clinical manifestations, and management strategies. It details various subtypes of JIA, their specific features, and the immunological and genetic factors involved in their pathogenesis. Additionally, the document emphasizes the importance of a multidisciplinary approach in managing JIA, including pharmacologic treatments, psychosocial support, and physical therapy to normalize joint function and prevent long-term complications.