Downloaded 155 times






























![M. Almuzian, January 2016 Universityof Sydney 44
GOLLEDGE, J. & ELLIS, H. 1994. The aetiology of lateral cervical (branchial) cysts: past and present
theories.TheJournalof Laryngology &Otology, 108, 653-659.
GRUELICH, W. & PYLE, I. 1959. A roentgenological atlas of skeletal maturation of the hand and wrist.
StanfordUniversityPress,Stanford,Calif.
HALL, B. K. 1988. The embryonicdevelopmentof bone. American Scientist,174-181.
HARTRIDGE, T., ILLING, H. & SANDY, J. 2014. The role of folic acid in oral clefting. British journal of
orthodontics.
JIANG, R., BUSH, J. O. & LIDRAL, A. C. 2006. Development of the upper lip: morphogenetic and
molecularmechanisms.DevelopmentalDynamics, 235,1152-1166.
LAMPARSKI, D. 1972. Skeletal age assessment utilizing cervical vertebrae [Master of dental science
thesis]. Pittsburgh:Universityof Pittsburgh,Schoolof DentalMedicine.
LU, C.-Y., TENG, R.-J., HOU, J.-W. & CHENG, T.-J. 1997. Bifid tongue associated with midline cleft
palate, mandible, cervical vertebrae and linea alba. European journal of pediatrics, 157, 86-
86.
MEIKLE, M. C. 1970. The effect of a Class II intermaxillary force on the dentofacial complex in the
adultMacaca mulattamonkey. American journalof orthodontics, 58,323-340.
MILLS, J. 1978. The effects of orthodontic treatment on the skeletal pattern. British journal of
orthodontics, 5,133.
MOSS, M. L. 1968. A theoretical analysisof the functional matrix. Acta Biotheoretica, 18,195-202.
MOSS, M. L. 1997a. The functional matrix hypothesis revisited. 1. The role of mechanotransduction.
American journalof orthodonticsand dentofacialorthopedics, 112, 8-11.
MOSS, M. L. 1997b. The functional matrix hypothesis revisited. 2. The role of an osseous connected
cellular network. American Journal of Orthodontics and dentofacial orthopedics, 112, 221-
226.
MOSS, M. L. & RANKOW, R. M. 1968. The Role of the Functional Matrix in Mandibular Growth*. The
Angleorthodontist, 38,95-103.
MOSS, M. L. & SALENTIJN, L. 1969. The capsular matrix. American journal of orthodontics, 56, 474-
490.
MRC VITAMIN STUDY RESEARCH, G. 1991. Prevention of neural tube defects: Results of the Medical
ResearchCouncil VitaminStudy. TheLancet, 338, 131-137.
NANDA, R. 1978. Protraction of maxilla in rhesus monkeys by controlled extraoral forces. American
journalof orthodontics, 74,121-141.
NANDA, R. S. & GHOSH, J. 1995. Longitudinal growth changes in the sagittal relationship of maxilla
and mandible. AmJOrthod DentofacialOrthop,107, 79-90.
PETROVIC, A. G., STUTZMANN, J. J. & OUDET, C. L. 1975. Control processes in the postnatal growth
of the condylar cartilage of the mandible. Determinants of mandibular form and growth.
Monograph, 4,101-53.
POSWILLO, D. 1975. The pathogenesis of the treacher Collins syndrome (Mandibulofacial dysostosis).
British Journalof Oral Surgery, 13, 1-26.
PROFFIT, W. R., FIELDS JR, H. W. & SARVER, D. M. 2014. Contemporary orthodontics, Elsevier Health
Sciences.
RAI, R., RAI, A. R., RAI, R., BHAT, K. & MURALIMANJU, B. 2012. Prevalence of bifid tongue and
Ankyloglossia in South Indian population with an emphasis on its embryogenesis. Int. j.
morphol, 30, 182-184.
SADLER, T. W. 2011. Langman'smedicalembryology,LippincottWilliams&Wilkins.
SARNAS, K. V. & SOLOW, B. 1980. Early adult changes in the skeletal and soft-tissue profile. Eur J
Orthod, 2, 1-12.
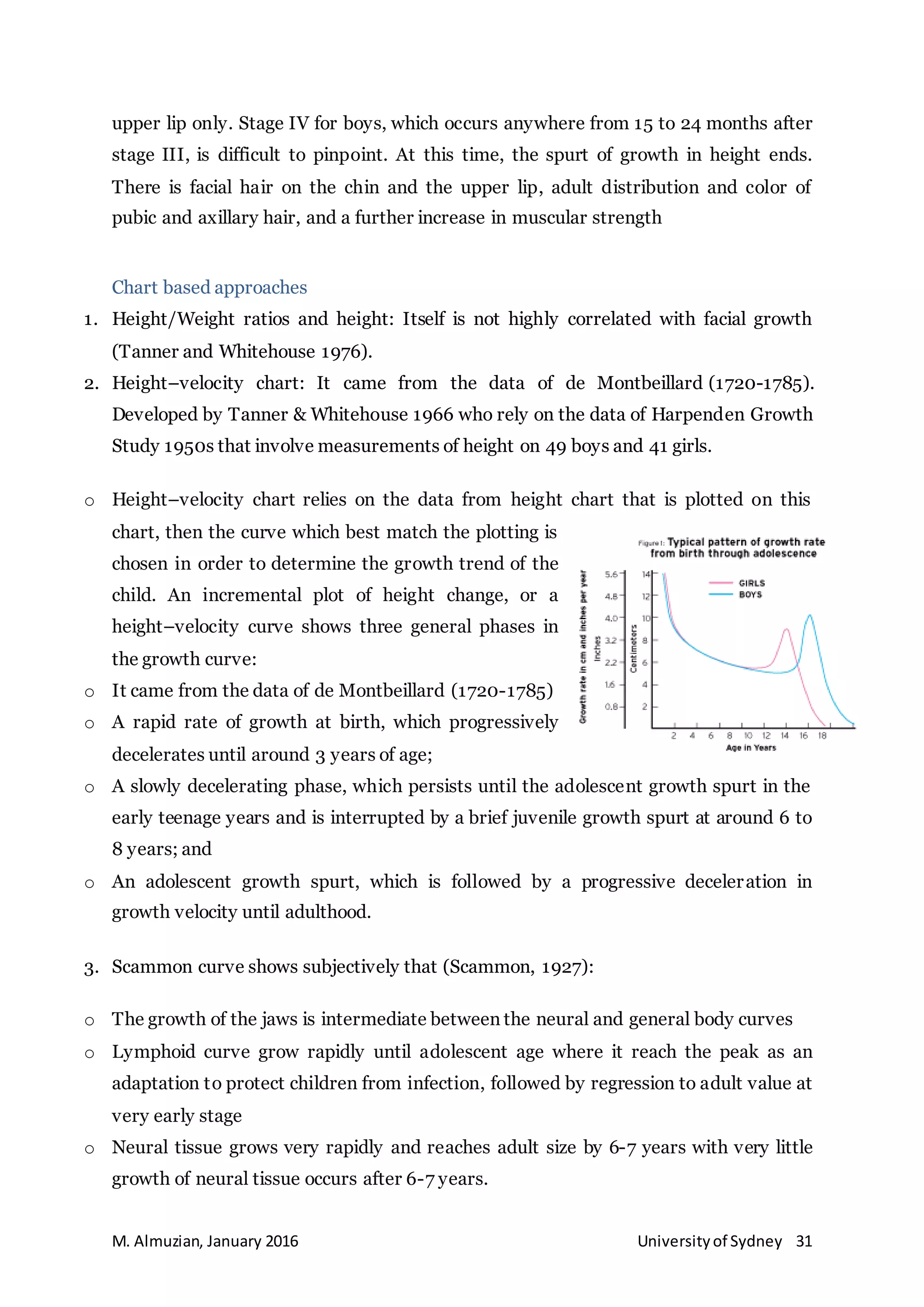
SCAMMON, R. E. 1927. The first seriatim study of human growth. American Journal of Physical
Anthropology, 10,329-336.
SCOTT, J. H. 1954. The growth of the human face. Proceedings of the Royal Society of Medicine, 47,
91.](https://image.slidesharecdn.com/growthdevelopmentbyalmuzianreadingnote-170314191133/75/Growth-development-for-orthodontists-by-Almuzian-44-2048.jpg)

This document provides an overview of craniofacial growth and development from embryological stages through postnatal growth. It describes the normal development from fertilization through formation of the germ layers and embryonic structures. Key structures like the pharyngeal arches and their derivatives are discussed. Theories of craniofacial growth and factors influencing growth such as genetics and nutrition are briefly introduced. The document serves as a lecture on applying embryological principles to understanding craniofacial development and orthodontics.











































































































