,
TEACHING
METHODS
A teaching methodis the way information is taught that brings the
learner into contact with what is to be learned. Examples of such
methods include lecture, group discussion, cooperative learning
strategies, one-to-one instruction, demonstration and return
demonstration, gaming, simulation, roleplay, role model, and self-
directed learning techniques. As the use of technology evolves, these
teaching methods also are being offered as blended opportunities by
integrating online and hybrid learning strategies ( Cook et al., 2008;
Johnson et al., 2012 ).
3.
When considering themany teaching methods available, the following
major factors should be take into account.
Audience characteristics (size, diversity, learning style preferences,
needs, abilities)
Educator's expertise as a teacher
Objectives of learning
Potential for achieving learning outcomes
Cost-effectivenessSetting for teaching
Evolving technology
4.
Lecture can bedefined as a highly structured method by
which the educator verbally transmits information directly to
a group of learners for the purpose of instruction. It is one of
the oldest and most often used approaches to teaching. The
word lecture comes from the medieval Latin term legere,
which means "to read" and the French word lecture, which
means "reading."
LECTURE
5.
2019), the followingapproaches enhance the effective transfer of
knowledge during a lecture.
Set goals by using opening and summary statements.
Be flexible.
Present key terms.
Offer examples.
Use analogies.
Use visual backups.
LECTURE
6.
Each lecture shouldinclude three main parts:
Introduction
Body
Conclusion
LECTURE
7.
Group discussion isdefined as a method of leaching whereby learners
get together to a Lively exchange information, ideas, feelings and
opinions with one another and with the educator. As an education sure
tsar effective teaching methodology for patient sa family education.
Group discussion provides not only a forum for the educator to share
information with there but also for pants to ask questions and
exchange thoughts, doubts, and experiences (Barros et al., 2018)
GROUP DISCUSSION
8.
Cooperative learning isa type of group teaching that uses group work
activities when teaching students and professionals belonging to a
variety of health disciplines. Group work is a learner-centered, active
(also known as transactional), and very effective teaching and earning
strategy for nursing students and staff to enhance their cognitive and
affective skills. In most instances, though, reaching and learning
activities related to group work sessions are not pertinent for patient
and family education.
COOPERATIVE LEARNING
9.
cooperative learning isa highly structured type of group work in that students
are supplied with information to read and analyze; the teacher is the center of
authority and observes, listens, and intervenes where necessary; students work
jointly as a team in an interactive and interdependent manner to build
foundational knowledge and problem solve in the process of completing an
activity or project; and individual students as well as the group as a whole submit
their work for assessment to receive prompt feedback on their performance as a
measure of success of intended learning. Teaching methods that use cooperative
learning strategies are applied mainly to the education of health professionals..
COOPERATIVE LEARNING
10.
Collaborative learning, onthe other hand, is unstructured; students find
their own sources of materials needed to carry out their role and
complete an activity, the teacher takes a hands-off approach and the
groups self-manage unless they ask for assistance, each student has a
different part to play in constructing knowledge (a constructivist approach
to discovering, understanding, and producing knowledge), and students
assess their own individual performance as well as their group's
performance (Brame & Biel, 2015; Davidson & Major, 2014; Tolsgaard et
al., 2016; Weimer, 2015).
COLLABORATIVE LEARNING
11.
Structured, evidence-based, innovativeteaching strategy meant
to engage students in active learning and enrich their
experiences by working together to achieve one or more
common learning objectives.
TEAM-BASED LEARNING (TBL)
12.
Associated with studentsacquiring knowledge and skills
through shared learning of matched equals. Instead of
professional teachers helping others to learn, students assist
each other to learn.
PEER-ASSISTED LEARNING (PAL)
13.
Requires students towork as individuals and as a team to
research critical and controversial issues or trends and then
present “pro” and “con” arguments in support of various points
of view.
DEBATE
14.
Method to stimulatelearners to gather and apply information to
solve problems based on realistic patient scenarios.
PROBLEM-BASED LEARNING (PBL)
15.
Student-centered method thatcan be used at different levels of
education (primary, high school, and college) and with different
disciplines to teach topics in classroom and workplace settings
(Moonaghi & Bagheri, 2017).
JIGSAW
16.
Group work strategiesinitiated by the instructor, who poses a
discussion question and gives students time to individually
think through a response or write an answer to the question.
THINK-PAIR-SHARE/WRITE-PAIR-SHARE
17.
Deliberate process thathelps individuals to consider their
experiences to gain insights and perspective about themselves
and their practice for the purpose of promoting their
provisional growth (Jootun, 2014).
SELF-REFLECTION
18.
Valuable teaching methodexperiential activities that provides
students with a reach and robust form of learning that takes
place in the community.
SERVICE LEARING
19.
Contemporary teaching methods,is a technique that uses
visual graphics (two-dimensional drawings or diagram) to help
student logically organized idea (concepts) and understand
relationship between topics.
CONCEPT MAPPING
20.
Also known ascase study or case method, is a method of
teaching that actively engages learners to focus on real or
invented case scenarios stimulating life or world situations to
understand and solve complex problems, dilemmas, or issues.
CASE-BASED LEARNING (CBL)
21.
Educational format thatconsists of one or several sessions in
which a small group of staff nurses or students, facilitated by
an educator, discusses issues that emerge from assigned
course content of practical relevance.
SEMINAR
22.
One-to-one instruction, whichmay be
given either formally or informally,
involves face-to-face delivery of
information specifically designed to meet
the needs of an individual learner.
ONE-TO ONE-INSTRUCTION
Thus, this one-to-one method of teaching,
also known as verbal instruction, is a
process of mutual interchange between
the patient and the health professional
(Marcus, 2014).
Formal one-to-one instruction is a
planned activity, whereas informal one-
to-one instruction is an unplanned
interaction.
23.
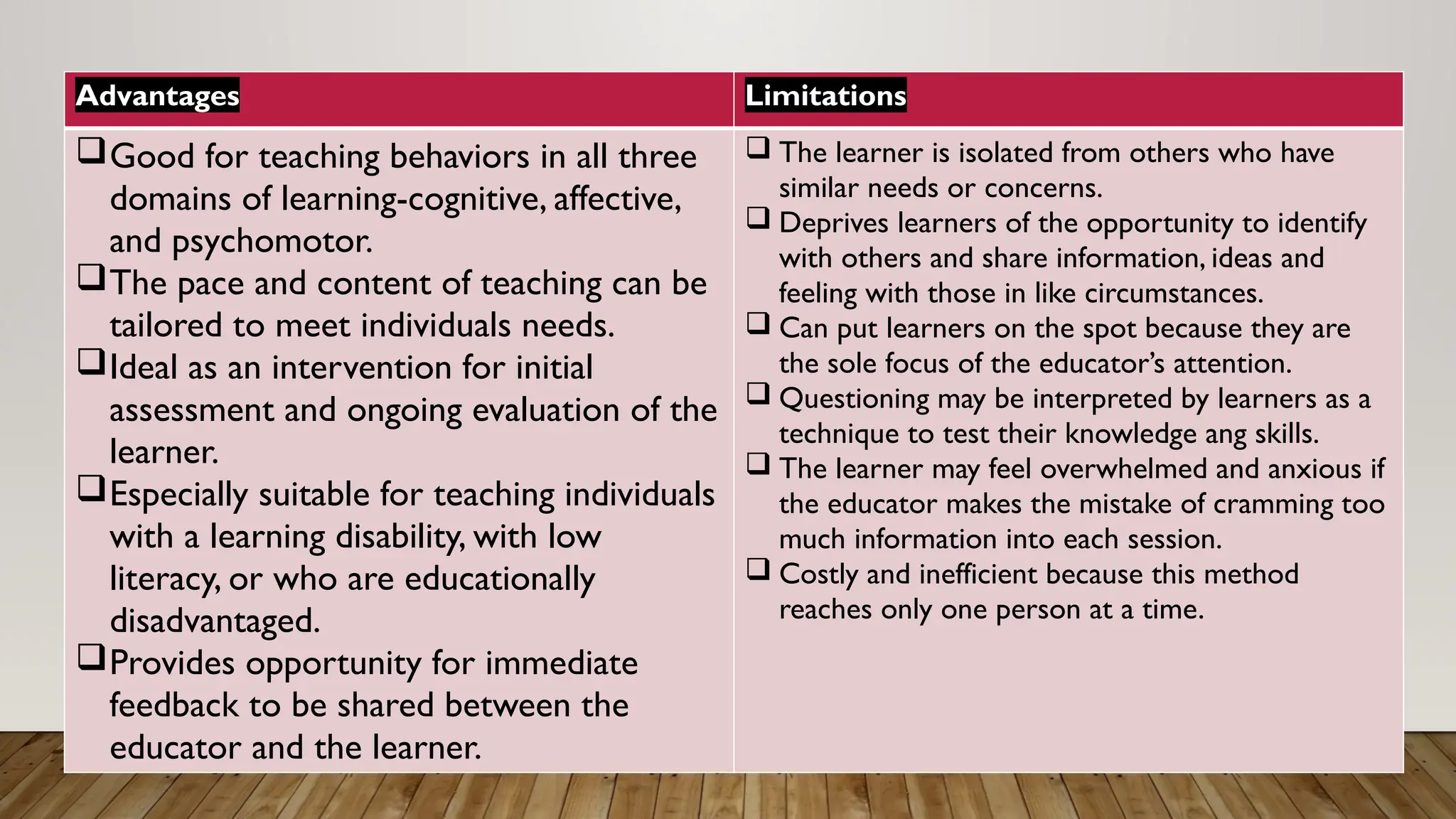
Advantages Limitations
Good forteaching behaviors in all three
domains of learning-cognitive, affective,
and psychomotor.
The pace and content of teaching can be
tailored to meet individuals needs.
Ideal as an intervention for initial
assessment and ongoing evaluation of the
learner.
Especially suitable for teaching individuals
with a learning disability, with low
literacy, or who are educationally
disadvantaged.
Provides opportunity for immediate
feedback to be shared between the
educator and the learner.
The learner is isolated from others who have
similar needs or concerns.
Deprives learners of the opportunity to identify
with others and share information, ideas and
feeling with those in like circumstances.
Can put learners on the spot because they are
the sole focus of the educator’s attention.
Questioning may be interpreted by learners as a
technique to test their knowledge ang skills.
The learner may feel overwhelmed and anxious if
the educator makes the mistake of cramming too
much information into each session.
Costly and inefficient because this method
reaches only one person at a time.
24.
Demonstration is doneby the educator to
show the learner how to perform a certain
skill. Return demonstration is carried out by
the learner as an attempt to establish
competence by performing a task with cues
from the educator as needed.
DEMONSTRATION AND RETURN
DEMONSTRATION
25.
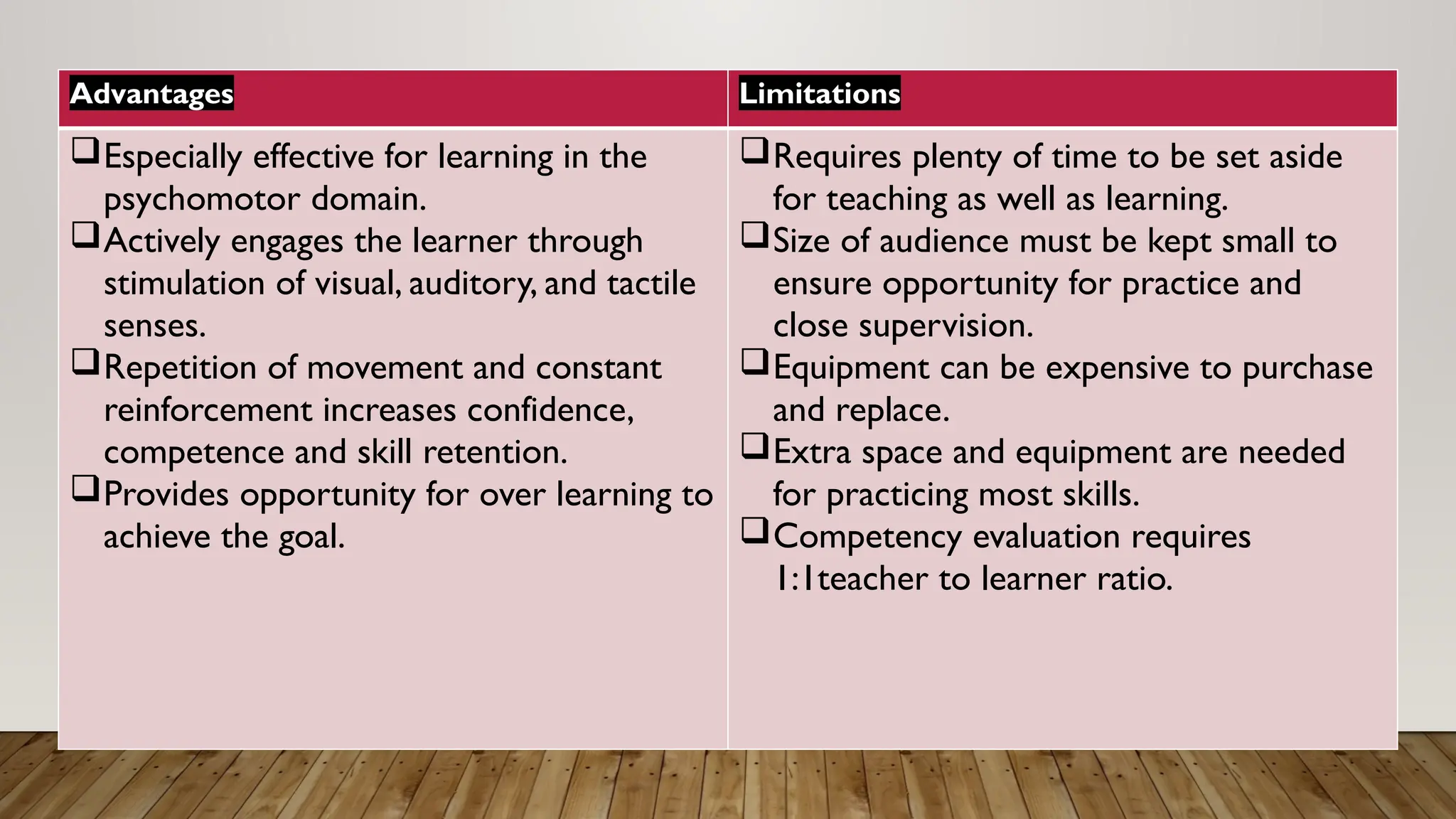
Advantages Limitations
Especially effectivefor learning in the
psychomotor domain.
Actively engages the learner through
stimulation of visual, auditory, and tactile
senses.
Repetition of movement and constant
reinforcement increases confidence,
competence and skill retention.
Provides opportunity for over learning to
achieve the goal.
Requires plenty of time to be set aside
for teaching as well as learning.
Size of audience must be kept small to
ensure opportunity for practice and
close supervision.
Equipment can be expensive to purchase
and replace.
Extra space and equipment are needed
for practicing most skills.
Competency evaluation requires
1:1teacher to learner ratio.
26.
Gaming is aninnovative method of
instruction requiring the learner to actively
participate in a competitive activity with
preset rules (Abigail, 2014, Allery, 2004).
Gamification is a process of adding games
or game elements to a teaching-learning
experience to enhance learner participation
by using rewards, badges or points for
completing a module (Gentry et al., 2019,
Shawaqfeh, 2015).
GAMING
27.
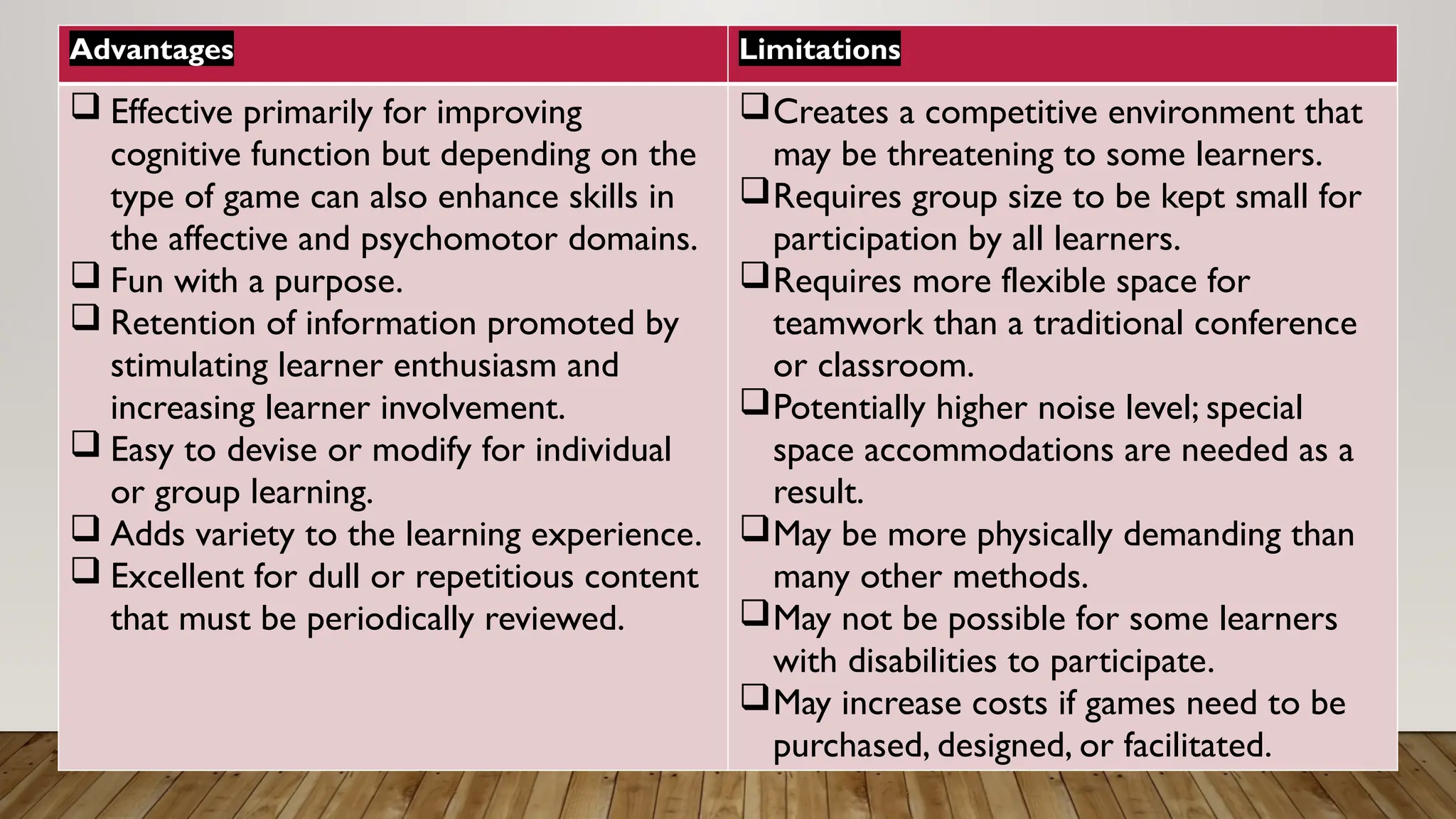
Advantages Limitations
Effectiveprimarily for improving
cognitive function but depending on the
type of game can also enhance skills in
the affective and psychomotor domains.
Fun with a purpose.
Retention of information promoted by
stimulating learner enthusiasm and
increasing learner involvement.
Easy to devise or modify for individual
or group learning.
Adds variety to the learning experience.
Excellent for dull or repetitious content
that must be periodically reviewed.
Creates a competitive environment that
may be threatening to some learners.
Requires group size to be kept small for
participation by all learners.
Requires more flexible space for
teamwork than a traditional conference
or classroom.
Potentially higher noise level; special
space accommodations are needed as a
result.
May be more physically demanding than
many other methods.
May not be possible for some learners
with disabilities to participate.
May increase costs if games need to be
purchased, designed, or facilitated.
28.
Simulation is atrial-and-error method of
teaching in which an artificial experience is
created that engages the learner in an activity
that reflects real-life conditions but with- out
the risk-taking consequences of an actual
situation.
SIMULATION
29.
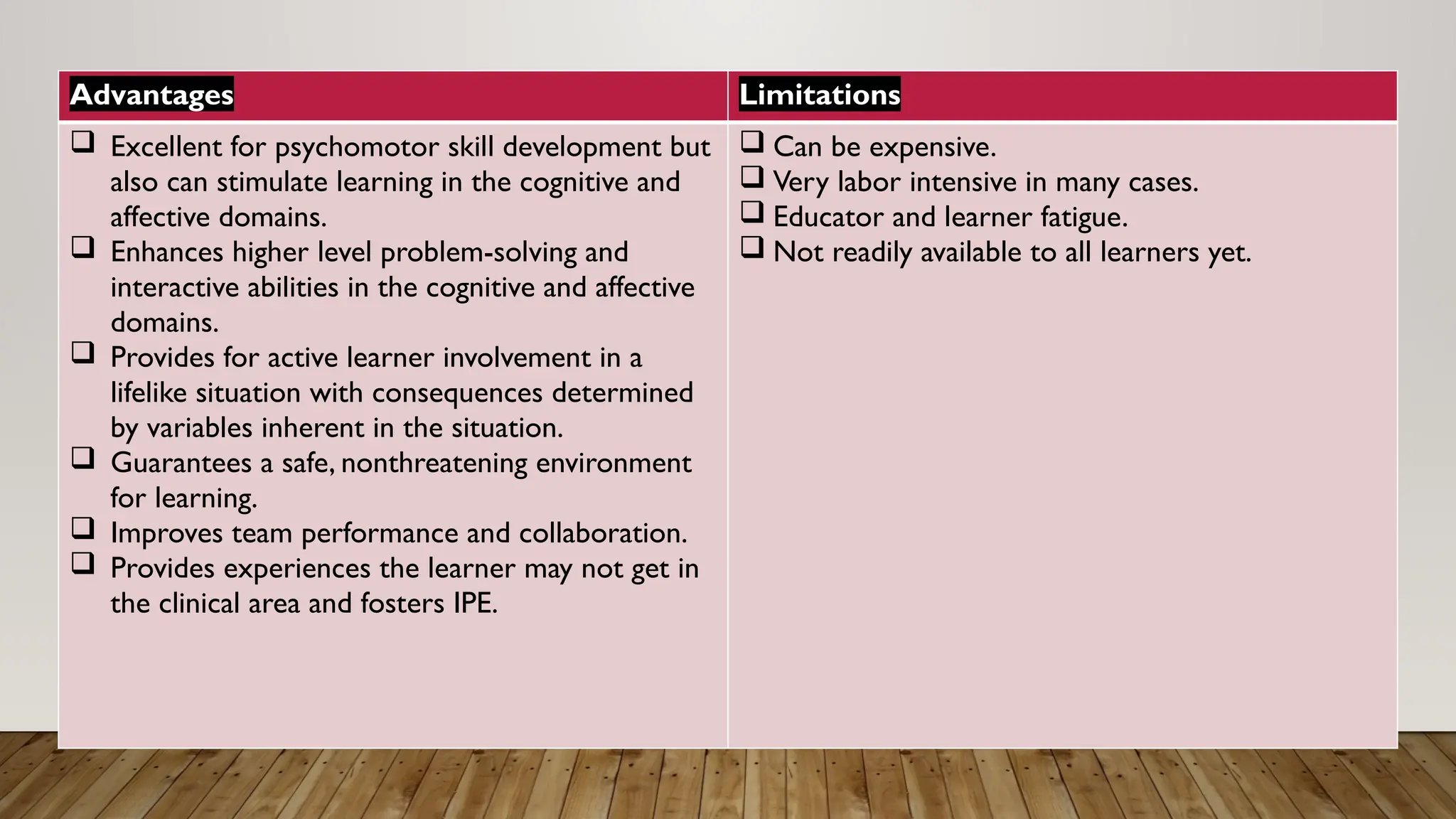
Advantages Limitations
Excellentfor psychomotor skill development but
also can stimulate learning in the cognitive and
affective domains.
Enhances higher level problem-solving and
interactive abilities in the cognitive and affective
domains.
Provides for active learner involvement in a
lifelike situation with consequences determined
by variables inherent in the situation.
Guarantees a safe, nonthreatening environment
for learning.
Improves team performance and collaboration.
Provides experiences the learner may not get in
the clinical area and fosters IPE.
Can be expensive.
Very labor intensive in many cases.
Educator and learner fatigue.
Not readily available to all learners yet.
30.
Role-play, sometimes alternativelyreferred to
as role-playing, is a method of instruction by
which learners actively participate in an
unrehearsed dramatization.
Participants are asked to play an assigned
character as they think the character would act
realistically. This technique is intended to
arouse feelings, elicit emotional responses,
and develop communication skills in the
learners.
ROLE-PLAY
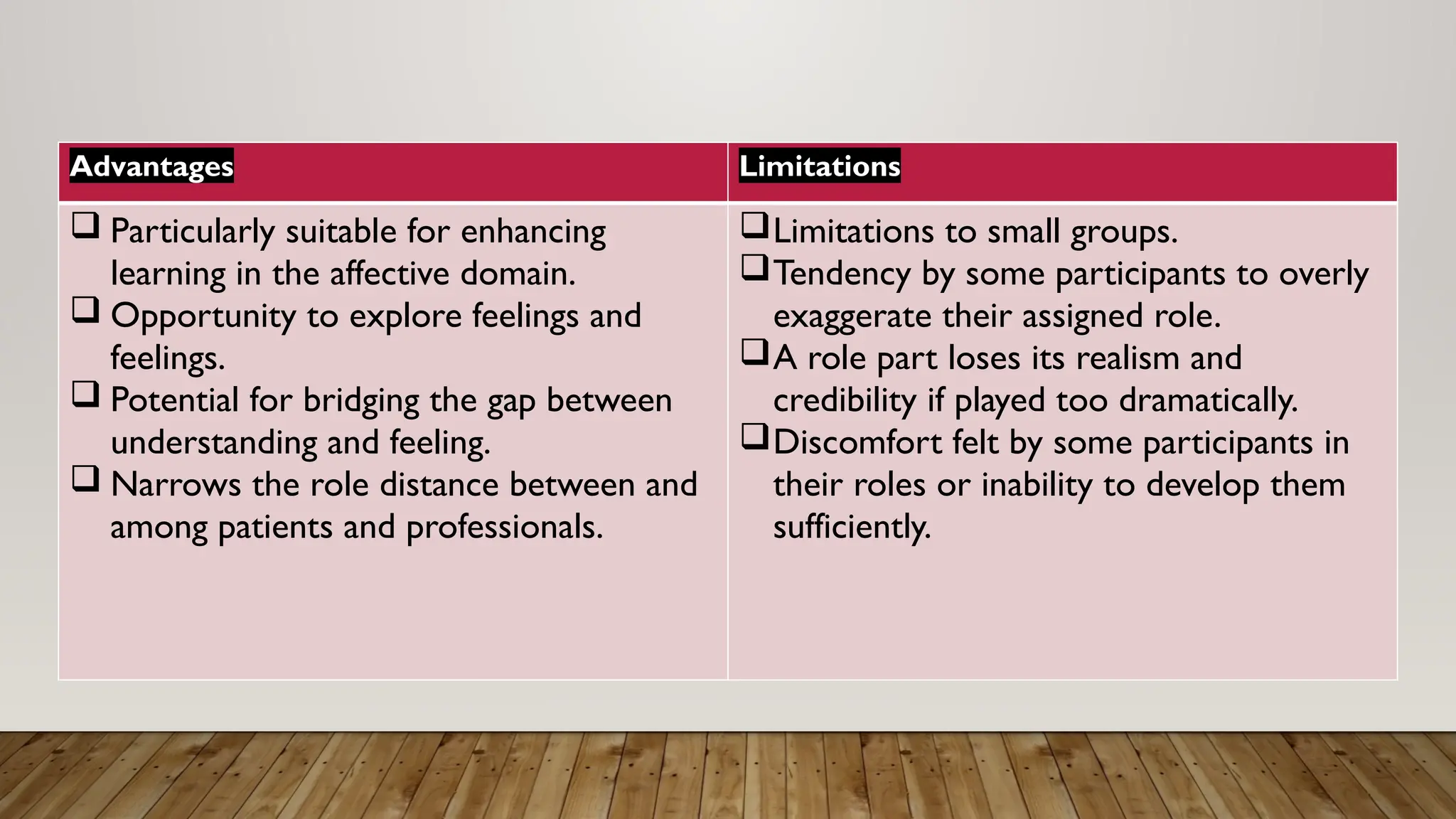
31.
Advantages Limitations
Particularlysuitable for enhancing
learning in the affective domain.
Opportunity to explore feelings and
feelings.
Potential for bridging the gap between
understanding and feeling.
Narrows the role distance between and
among patients and professionals.
Limitations to small groups.
Tendency by some participants to overly
exaggerate their assigned role.
A role part loses its realism and
credibility if played too dramatically.
Discomfort felt by some participants in
their roles or inability to develop them
sufficiently.
32.
A role modelis defined as someone whom
others look to as an example of behavior and/
or success to be imitated-a person to be
emulated.
Role model is a teaching method that can help
new health professionals develop critical
thinking competencies and interpersonal
skills, as well as assist them to assume the
responsibilities and values of the profession
with which they identify (Cruess et al., 2008;
Joneja & Sandhu, 2011; Sorensen & Yankech,
2008).
ROLE-MODEL
33.
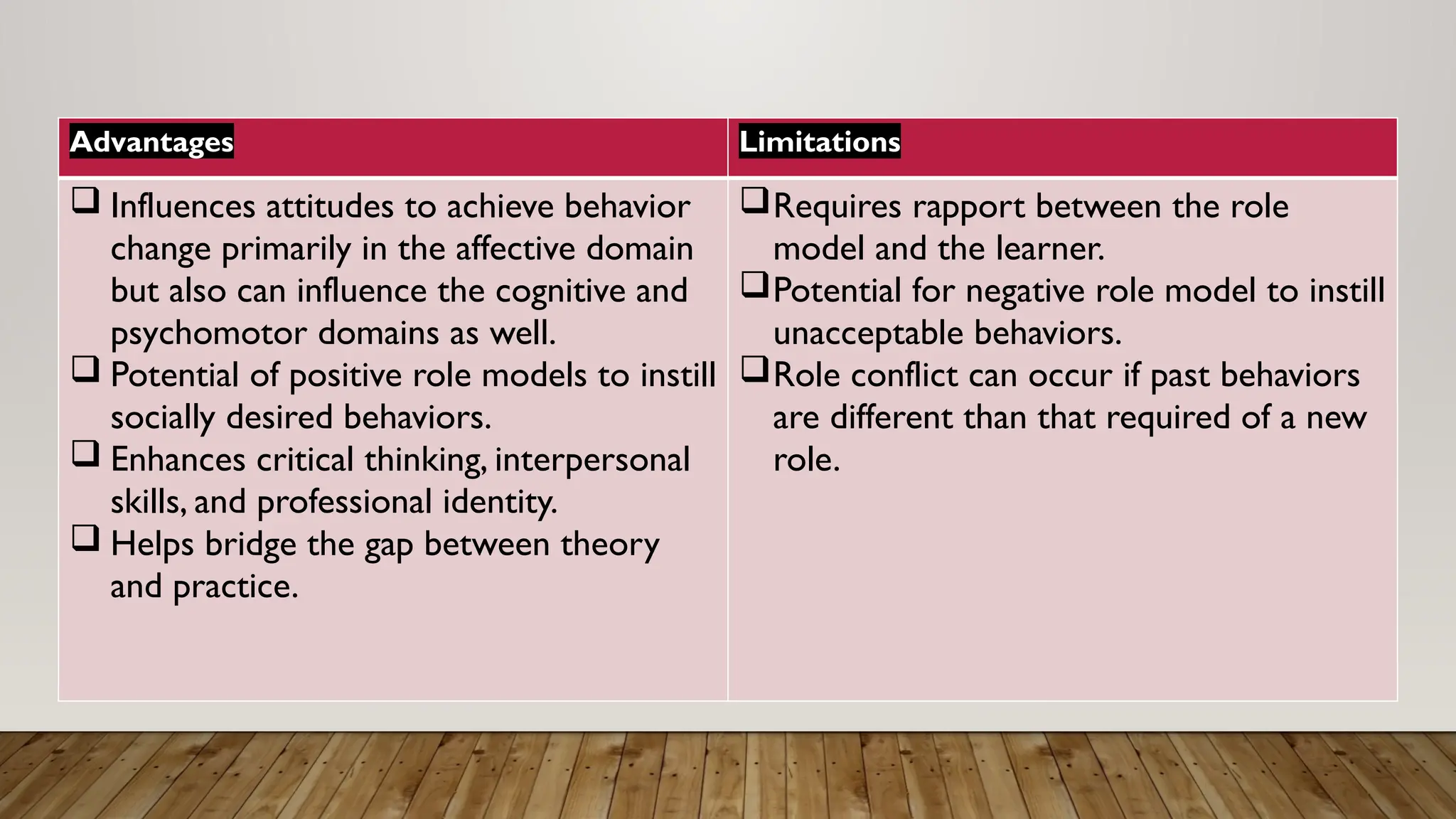
Advantages Limitations
Influencesattitudes to achieve behavior
change primarily in the affective domain
but also can influence the cognitive and
psychomotor domains as well.
Potential of positive role models to instill
socially desired behaviors.
Enhances critical thinking, interpersonal
skills, and professional identity.
Helps bridge the gap between theory
and practice.
Requires rapport between the role
model and the learner.
Potential for negative role model to instill
unacceptable behaviors.
Role conflict can occur if past behaviors
are different than that required of a new
role.
34.
Remote learning, alsocommonly referred to as
online learning, distance learning. e-learning,
web-based learning, distance education, and
virtual learning, is an ideal way to maximize
resources and to transmit current information
to people separated by space and time.
Through this strategy, the cost, time, and
inconvenience of travel no longer can keep an
audience from meeting face-to-face with an
expert (Cook et al., 2008; DeGolia, 2016).
REMOTE LEARNING
35.
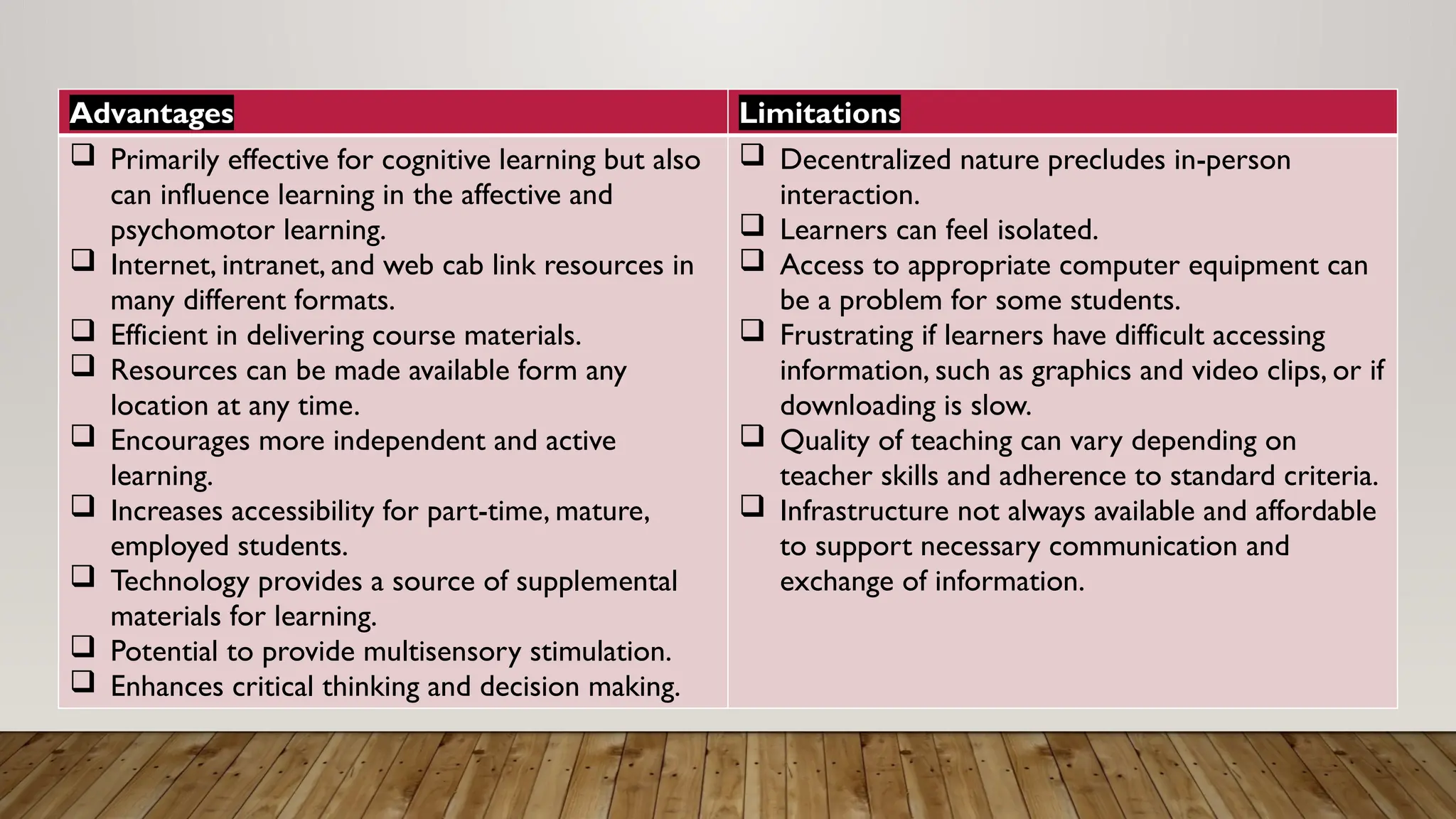
Advantages Limitations
Primarilyeffective for cognitive learning but also
can influence learning in the affective and
psychomotor learning.
Internet, intranet, and web cab link resources in
many different formats.
Efficient in delivering course materials.
Resources can be made available form any
location at any time.
Encourages more independent and active
learning.
Increases accessibility for part-time, mature,
employed students.
Technology provides a source of supplemental
materials for learning.
Potential to provide multisensory stimulation.
Enhances critical thinking and decision making.
Decentralized nature precludes in-person
interaction.
Learners can feel isolated.
Access to appropriate computer equipment can
be a problem for some students.
Frustrating if learners have difficult accessing
information, such as graphics and video clips, or if
downloading is slow.
Quality of teaching can vary depending on
teacher skills and adherence to standard criteria.
Infrastructure not always available and affordable
to support necessary communication and
exchange of information.
36.
Self-directed learning, alsocommonly
referred to as self-instruction, is a learner-
centered teaching method used by the
educator to provide or design instructional
activities that guide the learner in
independently achieving the objectives of
learning.
SELF-DIRECTED LEARNING
37.
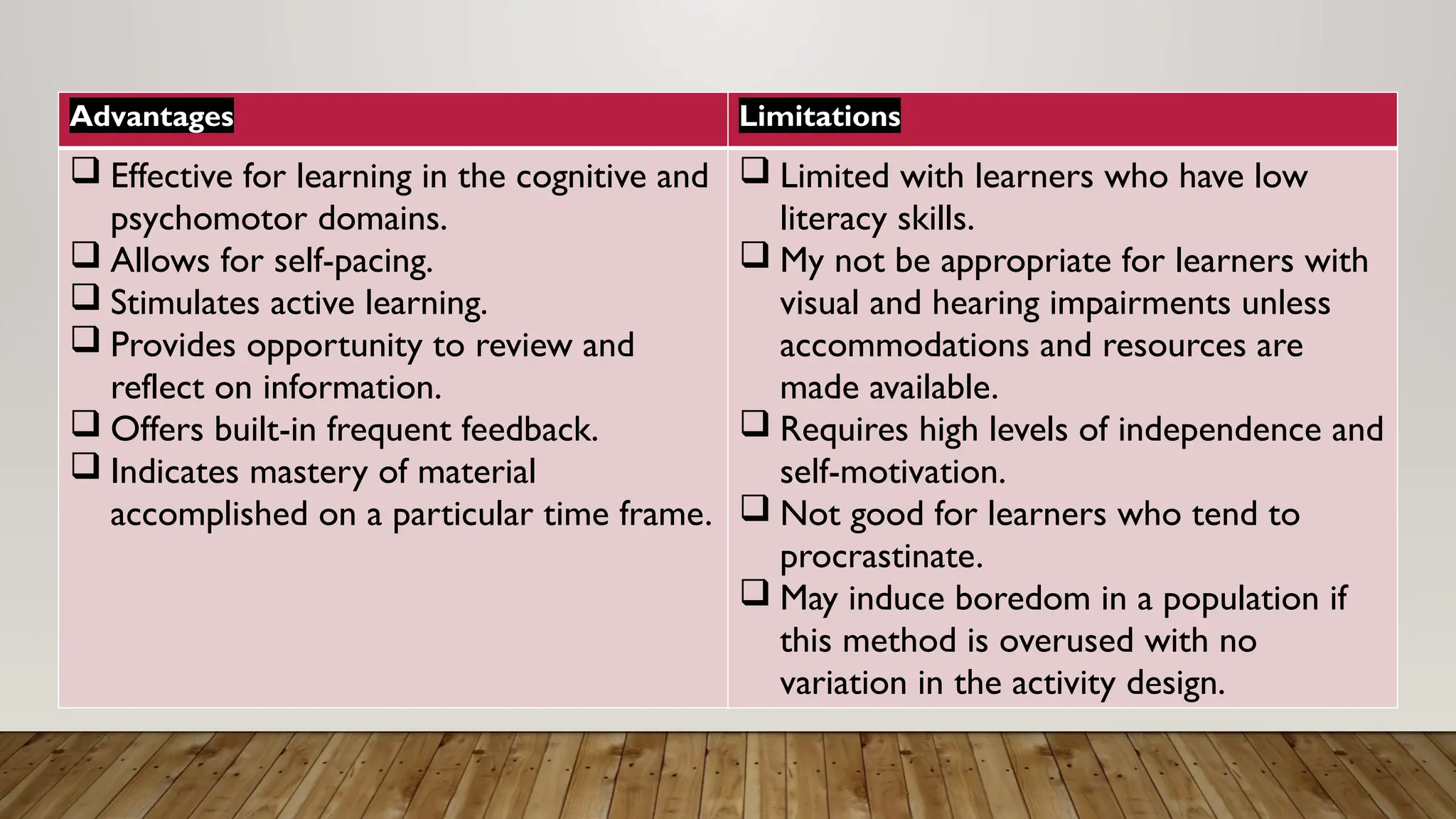
Advantages Limitations
Effectivefor learning in the cognitive and
psychomotor domains.
Allows for self-pacing.
Stimulates active learning.
Provides opportunity to review and
reflect on information.
Offers built-in frequent feedback.
Indicates mastery of material
accomplished on a particular time frame.
Limited with learners who have low
literacy skills.
My not be appropriate for learners with
visual and hearing impairments unless
accommodations and resources are
made available.
Requires high levels of independence and
self-motivation.
Not good for learners who tend to
procrastinate.
May induce boredom in a population if
this method is overused with no
variation in the activity design.
• Educator Self-Assessment
aprocess where educators reflect on their own
teaching practices, strength, and weaknesses to
improve their teaching skills.
• Evaluation of teaching Methods
A systematic process to assess the effectiveness of
teaching methods, including their impact on student
learning outcomes.
40.
• Characteristics ofa GreatTeacher
1. Present Information Enthusiastically- Delivering
information in a way that engages and motivates students.
2. Maintains Professionalism- Demonstrating expertise,
respect, and empathy in teaching practices.
3. Projects an Attitude of Caring- Showing genuine interest
and concern for students’ well-being and learning.
4. Exhibit Flexibility and Risk-taking Behavior- Being
adaptable and willing to try new teaching approaches.
5. Delivers Material Dramatically- Using creative and
engaging methods to present information.
41.
6. Sets HighExpectation- Encouraging students to strive
for excellence.
7. Serves as a role Model- Modeling behaviors and values
that promote healthy lifestyles.
8. Uses Anecdotes and Examples- Using real-life stories
and examples to illustrate key concepts.
9.Takes Advantage ofTechnology- Leveraging digital tools
to enhance teaching and learning.
10. Give Positive Reinforcement- Providing
encouragement and feedback to motivate students.
42.
11. Is Organizedand gives direction- Providing clear
instructions and guidance.
12. Uses Humor- Using humor to engage and relax students.
13. Elicits Feedback- Encouraging students to provide
feedback and suggestions.
14. UsesTeach-back- Checking students’ understanding by
asking them to explain key concepts.
15. Uses Repetition and Pacing- Adjusting teaching pace
and repeating key concepts to ensure student understanding.
43.
• Setting forTeaching
1.Healthcare Setting- Teaching in hospitals, clinics, and
other healthcare facilities.
2. Healthcare-related Setting- Teaching in nursing homes,
assisted living facilities, and other settings related to
healthcare.
3. Non-Healthcare Setting- Teaching in community
centers, school, and other settings outside of healthcare.
44.
• Sharing ResourcesAmong Settings
Collaborating and sharing resources across different
teaching settings to enhance teaching and learning.
• State of the Evidence
Using research and evidence-based practices to
inform teaching methods and improve student
learning outcomes.















![2nd yr bsc[n] cet ppt-methods of teaching -nsg education](https://cdn.slidesharecdn.com/ss_thumbnails/2ndyrbscncet-ppt-methodsofteaching-nsgeducation-200426055039-thumbnail.jpg?width=640&height=640&fit=bounds)








































