This document discusses ankle fractures in children. It provides details on:
1) The unique anatomy of the child's ankle including the physis and its development over time.
2) Common fracture patterns seen in children of different ages depending on the stage of osseous development.
3) The importance of achieving adequate reduction and protecting the physis to avoid growth alterations or deformities.
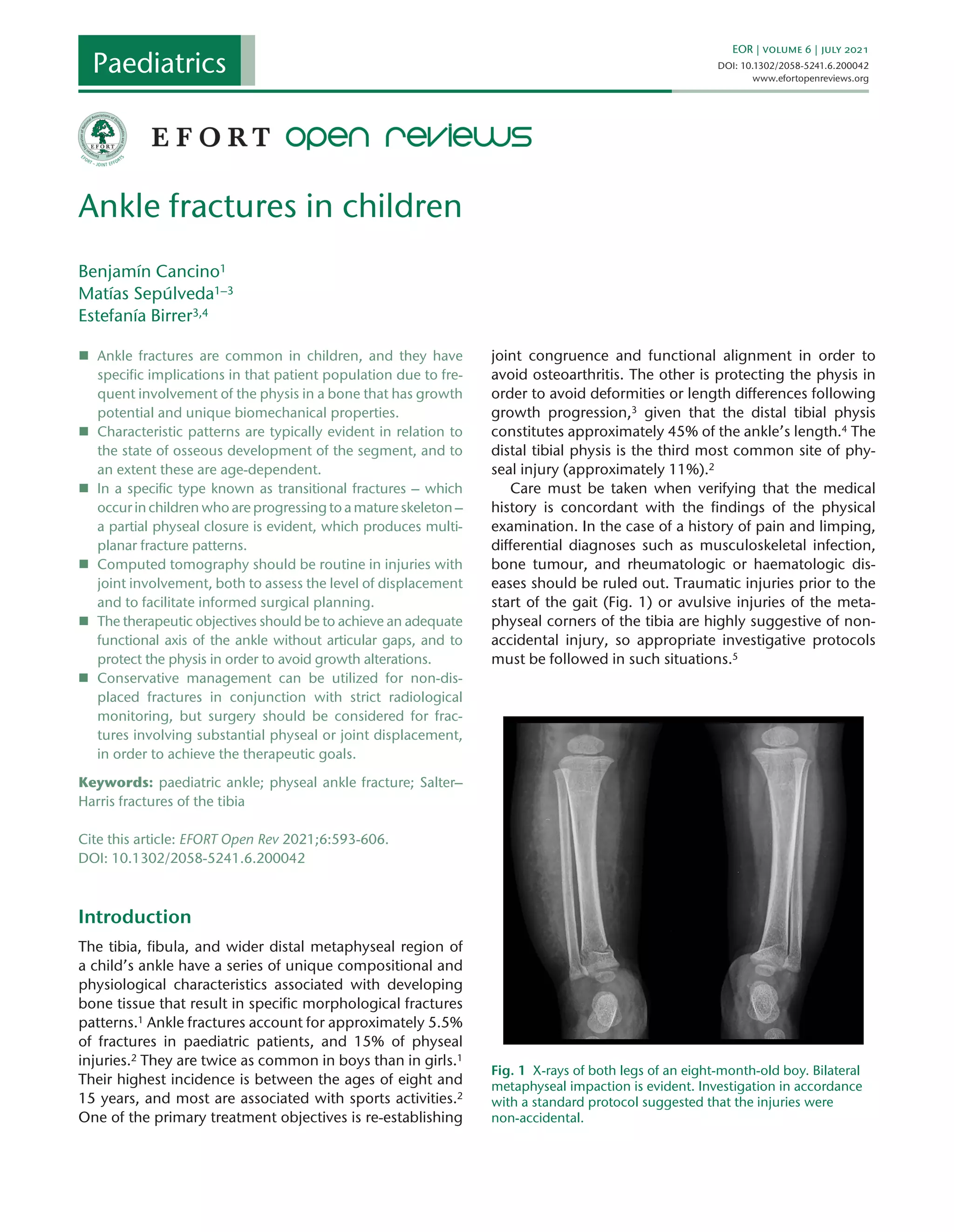
4) Guidelines for diagnosis including physical exam, imaging like x-rays and CT, and classifications systems like Salter-Harris that influence treatment and prognosis.