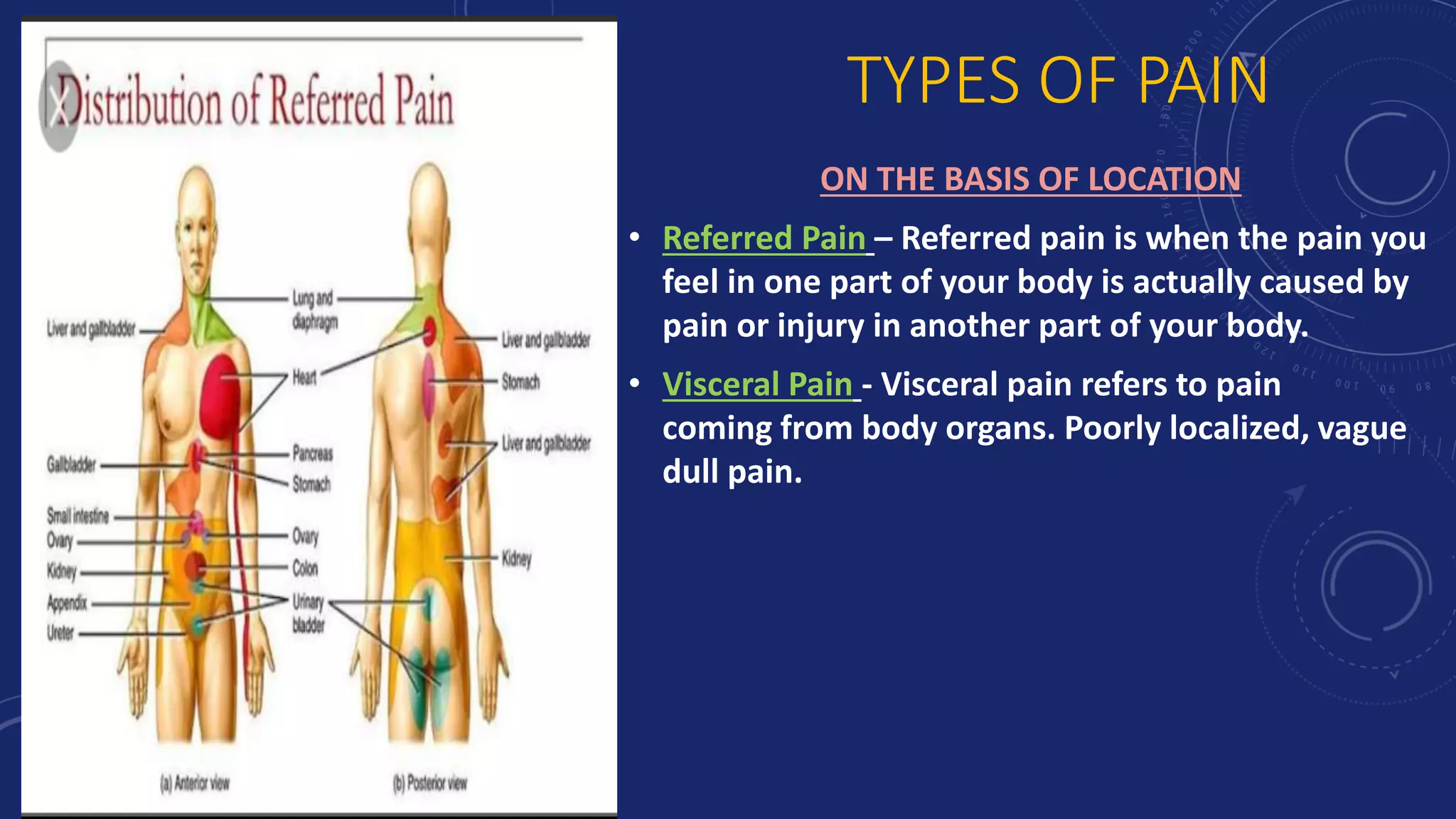
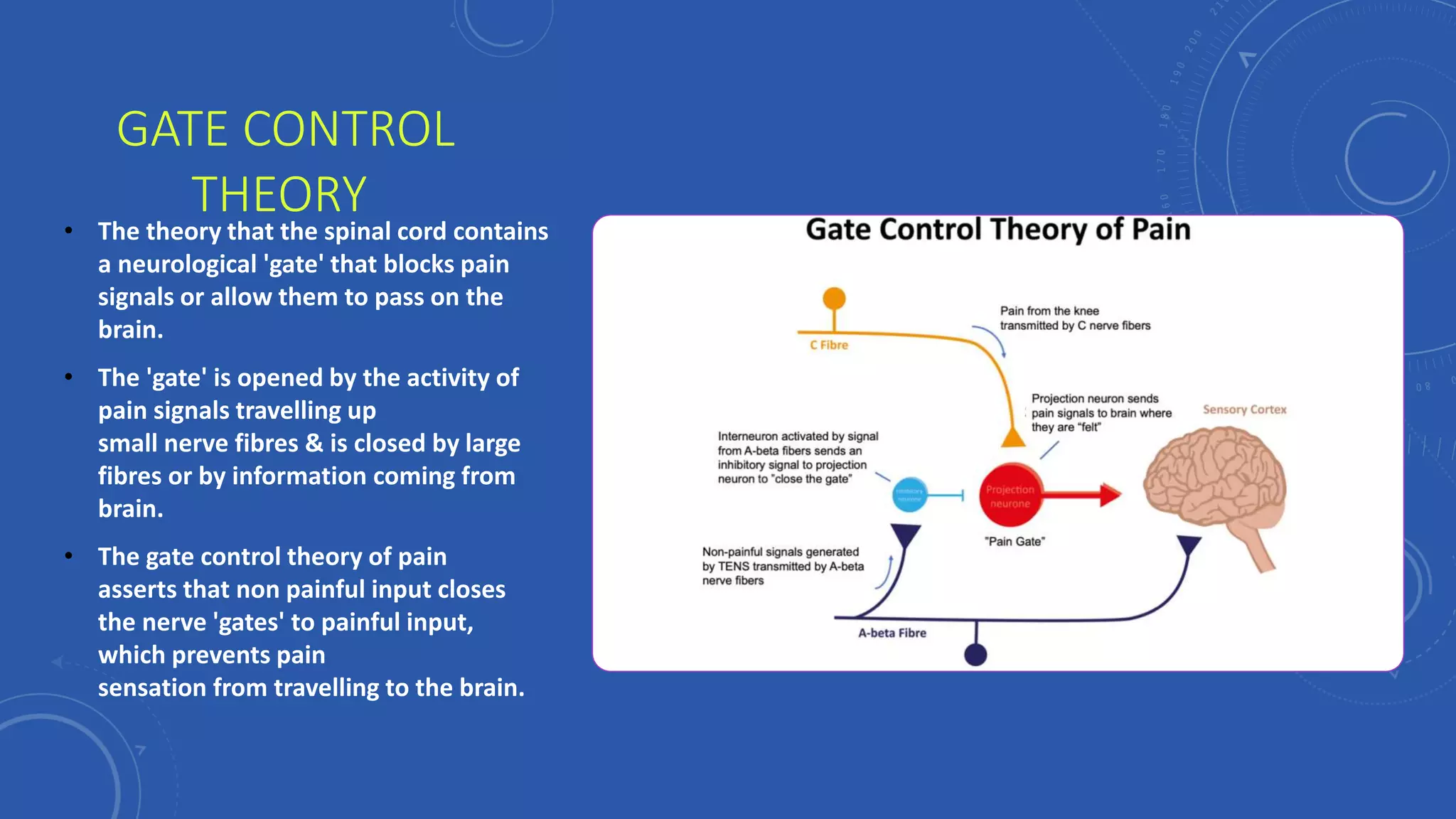
This document discusses pain management. It defines pain and describes the types of pain, including referred pain, visceral pain, acute pain and chronic pain. It also discusses factors that affect the perception of pain, such as age, fatigue, genes, and psychological factors. The document outlines the pathophysiology of pain, including nociceptors, the four phases of nociceptor activation, and the pathway of pain transmission. It also discusses theories of pain modulation, like the gate control theory. The final sections cover pain assessment, pharmacological and non-pharmacological management of pain, and sample nursing care plans.