• INTRODUCTION
• EVIDENCEFOR ROLE OF GENETICS IN PERIODONTICS
• BASIC TERMINOLOGIES
• POLYMORPHISM VS MUTATION
• GENETIC STUDY DESIGNS
• SYNDROME IN ASSOCIATION WITH PERIODONTAL
DISEASE
• GENETICS IN RELATION TO DISEASE
• GENE ASSOCIATION TO PERIODONTITIS
• FUTURE ASPECTS
• CONCLUSION
• REFERENCES
CONTENTS
3.
• Periodontitis isa chronic inflammatory disease of the supporting tissues of
the teeth. In subjects susceptible to destructive periodontal disease, there is
an imbalance between the host’s immune system and the oral Bacteria.
• The host’s immune system changes over time and can be positively or
negatively influenced by lifestyle.
• It was determined that around 38-82% of the clinical severity of the disease
was explained by genetic factors.(Michalowicz et.al 1991)
INTRODUCTION
Lindhe’s Clinical Periodontology & Implant Dentistry 7th
Ed
4.
• Genetic elementsplay a vital role in influencing the
inflammatory and immune response of the periodontal disease
• Genetic diseases are broadly classified into two entities.
INTRODUCTION
Simple Mendelian
Disorders
Complex Genetics
Disorder
Taba Jr M, Souza SL, Mariguela VC. Periodontal disease: a genetic perspective. Brazilian oral
research. 2012;26(spe1):32-8.
5.
EVIDENCE OF ROLEOF GENETICS IN PERIODONTITIS
• In a population in Sri Lanka without access to dental care and absence of
oral hygiene,Löe et al. (1986) were able to identify three subpopulations:
a group with no progression (11%), a group with moderate progression
(81%), and a group with rapid progression of periodontal breakdown
(8%).
• Van der Velden et al. 2006 found that 20% of the subjects developed
severe breakdown, whereas the remaining population developed minor-
to-moderate breakdown, and suggested that not everybody is equally
susceptible to periodontitis. This shaped the hypothesis that host
susceptibility may have a genetic background
Lindhe’s Clinical Periodontology & Implant Dentistry 7th
Ed
6.
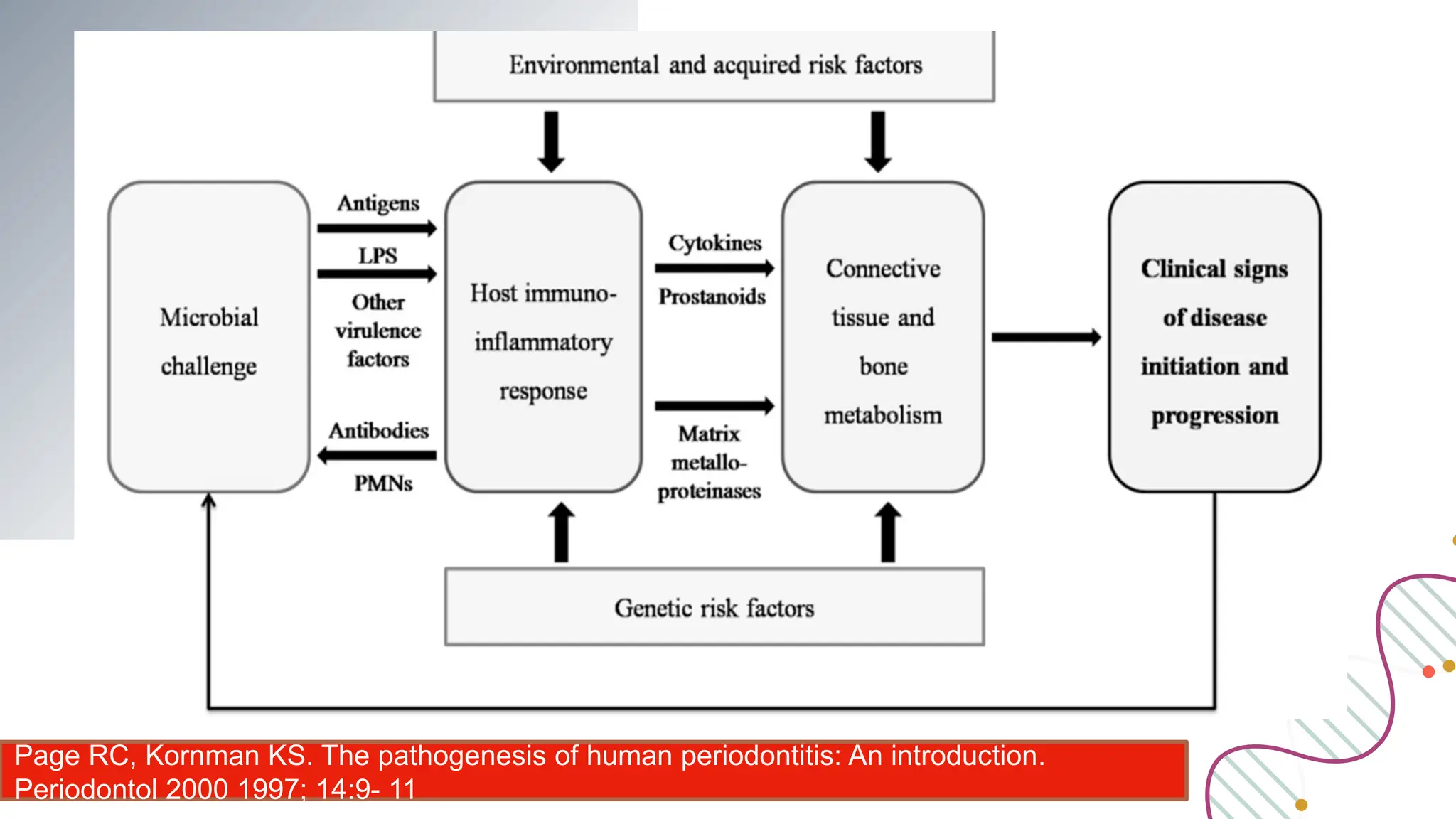
Page RC, KornmanKS. The pathogenesis of human periodontitis: An introduction.
Periodontol 2000 1997; 14:9- 11
DNA contains thegenetic code
The genetic code is read in groups of three nucleotides; each trinucleotide
sequence (triplet) is called a codon.
Written in the conventional direction from left to right.
Lindhe’s Clinical Periodontology & Implant Dentistry 7th
Ed
11.
A gene consistsof two parts :
(1) a coding region, i.e. a reading frame starting at nucleotide
position +1, containing a multitude of triplets that codes for a
sequence of amino acids to form a protein; and
(2) a promoter region, i.e. a sequence of nucleotides upstream (left)
of the coding region starting with nucleotide position -1. Within the
coding region intermittent areas of non-coding DNA exist; these
regions are called introns. The true coding areas within the coding
region are called exons
Lindhe’s Clinical Periodontology & Implant Dentistry 7th
Ed
GENETIC STUDY DESIGNS
Thestudies that show evidence of genetic predisposition to
periodontitis can be grouped into four areas of research
based on the statistical approaches to determine genetic
components and genetic model
Family studies Segregation analysis.
Linkage studies Association studies
Population studies
Twin studies
14.
● Familial aggregationcould result from shared genes, shared
environmental exposures and behavioural risk factors like education,
socio economic grouping, oral hygiene, possible transmission of
bacteria, diseases like polygenic disorder, passive smoking, exposure
to pollutants and sanitation.
● Therefore, the complex interactions between genes and also the
surroundings should even be thought-about in the analysis of familial
risk for periodontic diseases
FAMILY STUDY
Kinane DF, Hart TC. Genes and gene polymorphisms associated with periodontal disease.
Crit Rev Oral Biol Med 2003;14(6):430-449
15.
This longitudinal interventionalcase–control study aimed to evaluate the impact of parental periodontal
disease on the acquisition of oral pathogens in their offspring. Subgingival plaque and clinical periodontal
metrics were collected from 18 parents with a history of generalized aggressive periodontitis and their
children (6–12 years of age), and 18 periodontally healthy parents and their parents at baseline and
following professional oral prophylaxis.
Children of periodontitis parents were preferentially colonized by Filifactor alocis, Porphyromonas
gingivalis, Aggregatibacter actinomycetemcomitans, Streptococcus parasanguinis, Fusobacterium
nucleatum and several species belonging to the genus Selenomonas even in the absence of
periodontitis,
This study highlights the critical role played by parental disease in microbial colonization patterns in their
offspring and the early acquisition of periodontitis-related species and underscores the need for greater
surveillance and preventive measures in families of periodontitis patients.
17.
● Genes arepassed from parents to kids in an exceedingly
foreseeable manner, and typically segregate in families as
foretold by Mendel’s laws.
● Pattern of transmission of disease through generations is
analysed in several families and compared with those
expected under different models of inheritance to choose
the best fitting model.
SEGREGATION ANALYSIS
18.
● In thisway, segregation analysis helps to identify the best
model that simulates the ascertained transmission of a trait
in a given population by sequential comparison with all
the available models. Segregation analysis is applied by
geneticists to determine whether a trait transmission
belongs to Mendelian mode of genetic transmission
SEGREGATION ANALYSIS
19.
Advantages
Segregation analysis helpsto assess whether the disease gene is
autosomal or sex linked, recessive or dominant.
Limitations
1. Minimal power to resolve heterogeneity (Multiple causes)
2. Cannot distinguish between genetic and environmental influence
3. Does not find or aim to find a specific gene responsible for a trait.
20.
TWIN STUDIES
• Twinstudies are commonly used to study the
influence of genetic and environmental factors on the
complex diseases like periodontitis with multifactorial
aetiology.
• Sir Francis Galton in 1875 was the first scientist to
use this concept.
• The subject of interest in twin studies can be
monozygotic or dizygotic twins.
22.
Michalowicz BS, AeppliD,
Virag JG, et al. (1991)
Periodontal findings in adult
twins. J Periodontol
62:293–299.
23.
Therefore, the differencein concordance between MZ and DZ twins
for a specific phenotype could be used to evaluate the relative
contribution of genes (heredity) and environmental factors to a
disease and analysing disease presentation in twins is an essential
first step in this process.
Though twin studies overcame the drawbacks of segregation
analysis, few such studies have been conducted because of the
inadequacy of such twins.
24.
POPULATION STUDY
Environmental orbehavioural risk factors for a disease
are usually first detected in significant epidemiological
or population-based studies.
A genetic polymorphism is the long-time manifestation
in a population of two or more genotypes that could not
be maintained by frequent mutation.
Pihlstrom BL, Michalowicz BS, Johnson NW. Periodontal diseases. Lancet. 2005; 366(9499):
1809-1820
25.
1. The frequenciesof polymorphisms of candidate genes can be
compared between diseased individuals and controls . It can be
proved that the candidate gene determines the vulnerability to
disease when there is a clear cut difference in the frequency of a
specific polymorphism, between a case group and a control
group. In this way, pathogenesis, causal heterogeneity of disease
process and individuals most at risk for the disease can be
interpreted well.
POPULATION STUDY
Pihlstrom BL, Michalowicz BS, Johnson NW. Periodontal diseases. Lancet. 2005; 366(9499):
1809-1820
27.
1. Linkage analysisis a technique used to map the gene responsible
for a trait to a specific position on a chromosome.
2. The distance between two allele at different loci will determine
whether they will recombine. This is termed as recombination or
crossover event. There is 50% chance that any two maternal or
paternal alleles will recombine and be transmitted together to an
offspring.
3. Inheritance of a disease can be established if the distance
between marker and disease allele is within 20–30 centimo grams
(cM).
LINKAGE ANALYSIS
Boughman JA, Halloran SL, Roulston D, Schwartz S, Suzuki JB et al. An autosomal dominant form of periodontitis: its localization to
chromosome 4 and linkage to dentinogenesis imperfecta. J Craniofac Genet Dev Biol 1986; 6: 341-350.
29.
Test to comparethe likelihood that two loci are linked, vs the
likelihood that the two loci are unlinked.
LOD SCORE
Boughman JA, Halloran SL, Roulston D, Schwartz S, Suzuki JB et al. An
autosomal dominant form of periodontitis: its localization to chromosome 4 and
linkage to dentinogenesis imperfecta. J Craniofac Genet Dev Biol 1986; 6: 341-
31.
• Linkage studieshave been successful only in identifying the genetic basis of
simple Mendelian traits, where mutation of a single gene can cause a disease.
• Genetics and Periodontal Disease. Nevertheless, Linkage studies of complex
diseases are not successful since complex diseases are due to the combined
effect of multiple genes of minor effect and each gene contribute a small
amount to the disease phenotype
• It has extremely low statistical power for diseases in which there is extensive
heterogeneity among different families that have different combinations of
vulnerable genes and environmental exposures.
LIMITATIONS
32.
ASSOCIATION STUDY
Associations indicatethat the presence of an allele
confers risk for disease within a specific environment.
Allele association helps to identify whether the
frequency of an allele is considerably increased or
decreased in a particular disease
Schafer AS, Jepsen S, Loos BG. Periodontal genetics: a decade of genetic association studies
mandates better study designs. J Clin Periodontol 2011; 38(2): 103-107.
Schafer AS, JepsenS, Loos BG. Periodontal genetics: a decade of genetic association studies mandates
better study designs. J Clin Periodontol 2011; 38(2): 103-107.
Advantages-
Association studies are beneficial for discovery of inherited genetic variation
important for a wide range of complex diseases including diabetes, cardiovascular
diseases, metabolic disorders, obesity and mental illness.
Disadvantages
• In the presence of pathogens, individuals with the low response allele develop
disease. On the other hand, no relationship may exist between the disease and
this allele in populations where the particular bacteria is absent.
• • Low power to evaluate small genetic effects
• • Small presentation of actual causal or rare variants
1. Papillon-Lefèvre syndromeis a rare autosomal recessive
congenital disorder.
2. The gene responsible for this syndrome is cathepsin C, lysosomal
protease (Toomes et al. 1999).
3. The two essential features of Papillon-Lefèvre syndrome are
hyperkeratosis of the palms and soles (either diffuse or localized)
and generalized rapid destruction of the periodontal attachment
apparatus resulting in premature loss of both primary and
permanent teeth (Deas et al. 2003)
PAPILLON-LEFÈVRE SYNDROME
Ahuja V, Shin RH, Mudgil A, et al. (2005) Papillon-Lefèvre syndrome: A successful outcome. J
Periodontol 76:1996–2001.
39.
HAIM-MUNK SYNDROME
• Althoughthe palmoplantar findings and severe
periodontitis were suggestive of Papillon-Lefèvre
syndrome, the association of other clinical features,
particularly nail deformities and arachnodactyly, argued
that HaimMunk syndrome was a distinct disorder (Hart
et al. 1997)
• Hart et al. reported that the mutated gene of Haim-
Muck syndrome is cathepsin C.
Hart TC, Hart PS, Michalec MD, et al. (2000a) Haim-Munk syndrome and Papillon-Lefevre
syndrome are allelic mutations in cathepsin C. J Med Genet 37:88–94.
41.
EHLERS-DANLOS SYNDROME
1. Theprimary cause may be a type I or type II collagen deficiency,
a lysyl hydroxylase deficiency, deletion of N-telopeptide, or
disorders of copper homeostasis and fibronectin defects.
2. Radiographic appearance of a bulbous enlargement of the roots
together with pulp stones at other teeth were reported.
3. Early onset of periodontal disease, with premature loss of the
permanent teeth. Fragility of the alveolar mucosa and increased
bleeding tendencies have also been suggested (Badauy et al.
2007;
43.
CHEDIAK-HIGHACHI SYNDROME
1. Chediak-Higachisyndrome is a rare autosomal recessive
disease associated with impaired function of cytoplasmic
microtubules or microtubule assembly in PMNs (Oh et al.
2002).
2. The susceptibility to infections increases leads to early death
(often before 5 years of age) (Steenberghe 1997).
3. The disease reveals itself periodontally by severe gingivitis and
rapid loss of attachment, leading to exfoliation of the teeth
(Bailleul-Forestier et al. 2008; Steenberghe 1997).
44.
CYCLIC NEUTROPENIA
1. Cyclicneutropenia is a rare condition, characterized by cyclical
depletion of polymorphonuclear leukocyte numbers, typically in
3-week cycles, although this can be 5weeks.
2. Periodontal manifestations include inflamed gingival, gingival
ulceration, periodontal attachment, and bone loss (Kinane 1999;
Rezaei et al. 2004).
45.
1. Familial neutropeniais inherited as an autosomal dominant trait.
2. A slight monocytosis occurs, possibly as compensation, together
with the moderate neutropenia.
3. The condition is often diagnosed in patients with a history of
recurrent infections. Susceptibility to these infections tends to
vary with neutrophil count.
4. The periodontal manifestations include fiery red edematous
gingivitis, which is often hyperplastic and accompanied by
periodontal bone loss
FAMILIAL NEUTROPENIA
1. Cytokines suchas interleukin-1 (IL-1) and
tumor necrosis factor (TNF) have important
roles in bony destruction.
2. IL-1 family consists of at least three well-
studied genes: IL-1a and IL-1b, which have
agonist activity, and IL-1Ra, a physiologic
antagonist to the other IL-1 cytokines
INTERLEUKIN-1 GENE POLYMORPHISMS
51.
Interleukin-1 Genotype andExperimental Gingivitis
No evidence was provided that the IL-1 risk genotype was associated with higher
gingival crevicular fluid (GCF) volume and percentage bleeding on probing during the
development of experimental gingivitis (Jepsen et al. 2003).
Interleukin-1 Genotype and Chronic Periodontitis
Kornman et al. (1997) showed that a composite polymorphism of the IL-1A (at
position −889) and IL-1B (at position +3953) genes seems to cause an almost
sevenfold increased risk for progressive adult periodontitis in nonsmoking patients of
Caucasian origin.
INTERLEUKIN-1 GENOTYPE ANDAGGRESSIVE PERIODONTITIS
• With regard to the relationship between IL-1
genotype and aggressive periodontitis susceptibility,
conflicting results have been presented in different
ethnic populations.
Fiebig et al. (2008) conducted a casecontrol association study on 415
northern European Caucasian patients with aggressive periodontitis and 874
healthy controls to examine 10 single-nucleotide polymorphisms (SNPs) in
the genes of the IL1 cluster for association with IL1A, IL1B, CKAP2L
(cytoskeleton-associated protein 2-like), and IL1RN (IL-1 receptor
antagonist). It was concluded that the results do not support an association
between variants in the IL1 gene cluster and aggressive periodontitis.
55.
IL-10 gene polymorphisms
IL-10is located on chromosome 1, in a cluster with closely related
interleukin genes, including 1L-19, IL20 and IL-24. IL-10 plays a
role in the regulation of pro-inflammatory cytokines such as IL-1
and TNF-a. Functional disturbance in IL-10 due to genetic
polymorphisms could be detrimental to host tissues and could be
linked to periodontal disease susceptibility. IL-10 gene
polymorphisms have been investigated in relation to aggressive
periodontitis
Shimada Y, TaiH, Endo M, et al. (2004)
Association of tumor necrosis factor receptor
type 2 +587 gene polymorphism with severe
chronic periodontitis. J Clin Periodontol
31:463–469
58.
FC RECEPTOR POLYMORPHISMS
DijstelbloemHM, van de Winkel JG, Kallenberg CG (2001) Inflammation in autoimmunity: Receptors for IgG
revisited. Trends Immunol 22:510–516.
59.
FcgRIIa was shownto have two allelic forms: HR (high responder)
and LR (low responder). These names are based on the capacity of T
cells from normal individuals to proliferate in response to the
monoclonal antibody (IgG1) anti-CD3.
61.
● The genefor the CD14 receptor is on chromosome 5 (region
q23–21), encodes a protein of 375 amino acids.
● Data have shown the strong relevance of the CD14 receptor
activity in the clinical manifestation and development of
periodontitis.
● The systemic level of the soluble form of CD14 (sCD14) is
significantly increased in patients with periodontal disease
(Hayashi et al. 1999).
CD14 GENE POLYMORPHISMS
Folwaczny M, Glas J, Torok HP, Fricke K, Folwaczny C. The CD14-159C-to-T promoter
polymorphism in periodontal disease. J Clin Periodontol 2004;31:991-5
62.
CD14 gene polymorphisms
TheR-allele in the promoter region of CD14 at position -260(-159)
enhances the transcriptional activity of the gene.
A higher frequency of the N –allele and the N/N genotype of
CD14-1359 polymorphism was found in patients in severe
periodontitis.
Folwaczny M, Glas J, Torok HP, Fricke K, Folwaczny C. The CD14-159C-to-T promoter
polymorphism in periodontal disease. J Clin Periodontol 2004;31:991-5
63.
TLRs are importantinitiators of
innate immunity, recognizing diverse
microbial products which are
collectively known as pathogen-
associated molecular patterns
(PAMPs).
Toll like receptor, TLR2 and TLR4 Gene Polymorphisms
Barton GM, Medzhitov R (2004) Toll signaling: RIPping off the TNF pathway. Nat
Immunol 5:472–474
Schröder et al.(2005) reported that TLR-4 single-nucleotide
polymorphisms (Asp299Gly and Thr399Ile) were correlated with CP
(OR = 5.56, 95% CI: 2.19–14.04, P < 0.0001), but not with
aggressive periodontitis.
Fukusaki et al. (2007) revealed that the frequency of the C/C
genotype in TLR4 3725G > C polymorphism was significantly higher
in both the moderate and the severe periodontitis patient group than
in the control group
66.
MATRIX METALLOPROTEINASE POLYMORPHISMS
1.MMPs are one of the most important groups of
enzymes involved in periodontal connective tissue
destruction (Reynolds et al. 1994; Uitto et al. 2003).
2. It was demonstrated that the MMPs collagenase,
gelatinase A, stromelysin-1, and their specific
inhibitor TIMP-1 can all be detected in gingival
tissues by immunological assays, both from patients
with periodontitis and from patients undergoing
crown-lengthening procedures
69.
GENE THERAPY
Chatterjee, Singh,Nidhi; Saluja, Mini. Gene therapy in periodontics. Journal of Indian
Society of Periodontology 17(2):p 156-161, Mar–Apr 2013
1. Nutrigenomics isa new, rising feld of science that creates a
spider web connecting both nutrition and genome activity.
2. Nutrients ingested form the stimuli or the “dietary signals” that
are captured by the sensory systems in the cells and directly
impacting patterns of gene, protein and metabolite expressions.
3. Examples are -Cytochrome P450 enzymes and genes
Glutathione S-transferases (GSTs)
Methylenetetrahydrofolate reductase (MTHFR)
NUTRIGENOMICS
Neemat M. Kassem, Yassmin A. Abdelmegid, Mahmoud K. El-Sayed, Rana S. Sayed, Mahmoud H. Abdel-Aalla,
Hebatallah A. Kassem,Nutrigenomics and microbiome shaping the future of personalized medicine: a review
article,Journal of Genetic Engineering and Biotechnology,Volume 21,Issue1,2023,134
CONCLUSION
● With recentevidence implicating the role of periodontal
disease on systemic health, an understanding of the
potential role of genetic polymorphisms on periodontal
disease may help in modifying our treatment plan to
improve periodontal health, as well as, general health.
75.
REFRENCES
• Umesh, S.G. , Ramachandran, L. , Karthikeyan, J. , Mani, A. . Genetics and Periodontal
Disease: An Explicit Insight. In: Surlin, P. , editor. Periodontology - Fundamentals and
Clinical Features [Internet]. London: IntechOpen; 2021
• Wankhede AN, Wankhede SA, Wasu SP. Role of genetic in periodontal disease. J Int Clin
Dent Res Organ 2017;9:53-8.
• Genes and gene polymorphisms associated with periodontal disease; Crit Rev Oral Biol
Med:14(6):430-449 (2003)
• Kinane DF, Hart TC. Genes and gene polymorphisms associated with periodontal disease.
Crit Rev Oral Biol Med 2003;14(6):430-449
• Michalowicz BS, Diehl SR, Gunsolley JC, Sparks BS, Brooks CN, Koertge TE et al.
Evidence of a substantial genetic basis for risk of adult periodontitis. J Periodontol 2000;
71(11).):
• Folwaczny M, Glas J, Torok HP, Fricke K, Folwaczny C. The CD14-159C-to-T promoter
polymorphism in periodontal disease. J Clin Periodontol 2004;31:991-5
• 1699-1707
76.
REFRENCES
• Chatterjee, Singh,Nidhi; Saluja, Mini. Gene therapy in periodontics. Journal of Indian Society of
Periodontology 17(2):p 156-161, Mar–Apr 2013
• Barton GM, Medzhitov R (2004) Toll signaling: RIPping off the TNF pathway. Nat Immunol 5:472–
474.
• Taba Jr M, Souza SL, Mariguela VC. Periodontal disease: a genetic perspective. Brazilian oral
research. 2012;26(spe1):32-8.
• Pihlstrom BL, Michalowicz BS, Johnson NW. Periodontal diseases. Lancet. 2005; 366(9499): 1809-
1820
• Hart TC, Hart PS, Michalec MD, et al. (2000a) Haim-Munk syndrome and Papillon-Lefevre
syndrome are allelic mutations in cathepsin C. J Med Genet 37:88–94.
• Dijstelbloem HM, van de Winkel JG, Kallenberg CG (2001) Inflammation in autoimmunity:
Receptors for IgG revisited. Trends Immunol 22:510–516.
• Neemat M. Kassem, Yassmin A. Abdelmegid, Mahmoud K. El-Sayed, Rana S. Sayed,
Mahmoud H. Abdel-Aalla, Hebatallah A. Kassem,Nutrigenomics and microbiome
shaping the future of personalized medicine: a review article,Journal of Genetic
Engineering and Biotechnology,Volume 21,Issue1,2023,134









































































![REFRENCES
• Umesh, S. G. , Ramachandran, L. , Karthikeyan, J. , Mani, A. . Genetics and Periodontal
Disease: An Explicit Insight. In: Surlin, P. , editor. Periodontology - Fundamentals and
Clinical Features [Internet]. London: IntechOpen; 2021
• Wankhede AN, Wankhede SA, Wasu SP. Role of genetic in periodontal disease. J Int Clin
Dent Res Organ 2017;9:53-8.
• Genes and gene polymorphisms associated with periodontal disease; Crit Rev Oral Biol
Med:14(6):430-449 (2003)
• Kinane DF, Hart TC. Genes and gene polymorphisms associated with periodontal disease.
Crit Rev Oral Biol Med 2003;14(6):430-449
• Michalowicz BS, Diehl SR, Gunsolley JC, Sparks BS, Brooks CN, Koertge TE et al.
Evidence of a substantial genetic basis for risk of adult periodontitis. J Periodontol 2000;
71(11).):
• Folwaczny M, Glas J, Torok HP, Fricke K, Folwaczny C. The CD14-159C-to-T promoter
polymorphism in periodontal disease. J Clin Periodontol 2004;31:991-5
• 1699-1707](https://image.slidesharecdn.com/geneticsandperiodontaldisease-250227090600-3c63caf4/75/Genetics-and-their-effects-in-periodontal-disease-pptx-75-2048.jpg)





































































