This document discusses several types of bone diseases:
I. Hereditary bone diseases including familial fibrous dysplasia, osteogenesis imperfecta, and osteopetrosis.
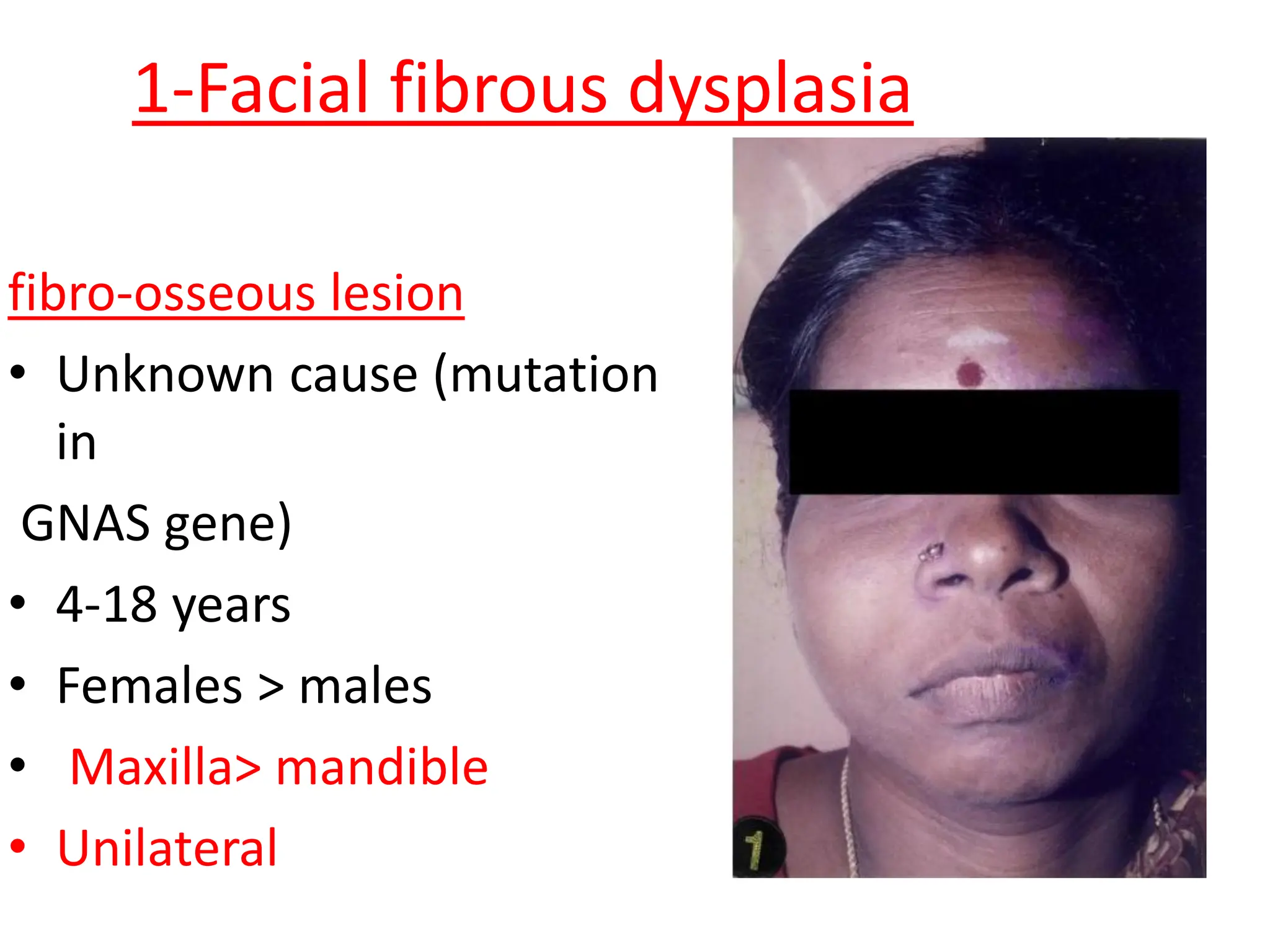
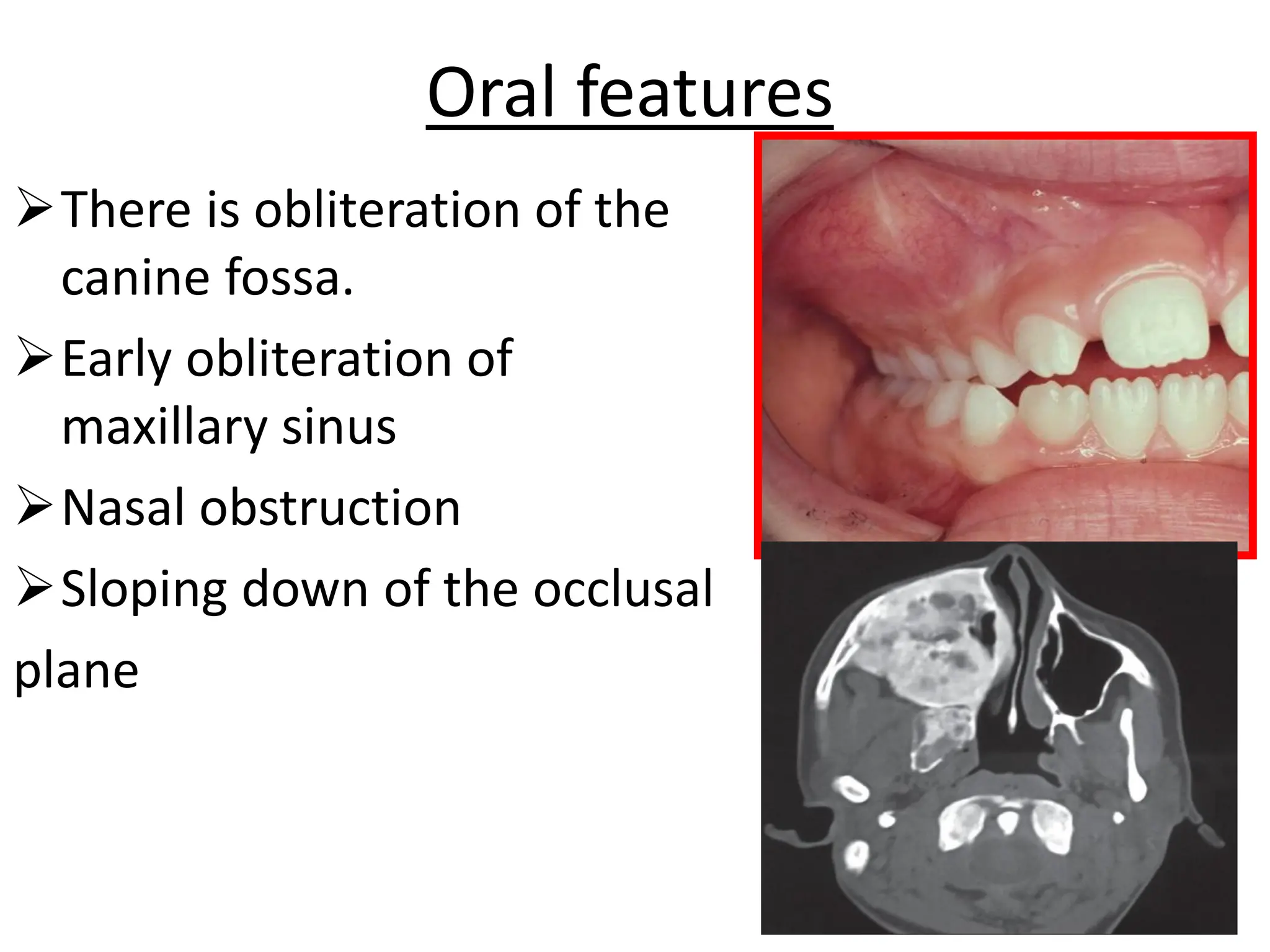
II. Acquired bone diseases such as facial fibrous dysplasia, Paget's disease, and hyperparathyroidism.
III. Neoplastic bone diseases including ossifying fibroma and central giant cell tumor. Key characteristics, clinical features, radiographic presentations, and histopathological findings of each disease are described.