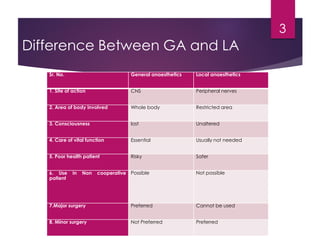
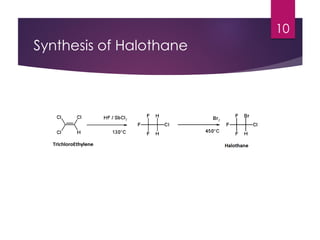
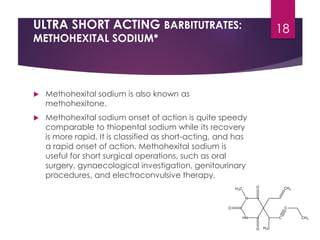
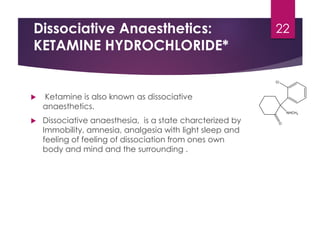
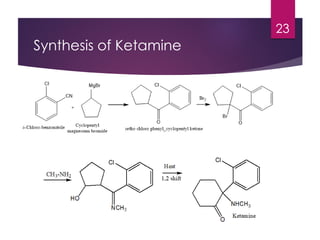
General anesthetics are drugs that produce reversible loss of sensation and consciousness. They are used during surgery to induce unconsciousness and abolish pain sensation. There are several stages of general anesthesia including analgesia, delirium, surgical anesthesia, and medullary paralysis. Common classes of general anesthetics include inhalational agents like halothane, methoxyflurane, enflurane, isoflurane, sevoflurane, and desflurane. Intravenous anesthetics include ultra short-acting barbiturates like thiopental sodium and methohexital sodium, as well as the dissociative anesthetic ketamine.




















![GENERAL_ANAESTHETICS[1] - Read-Only.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/generalanaesthetics1-read-only-241121061647-7b143b40-thumbnail.jpg?width=640&height=640&fit=bounds)













![anti diabetics [Autosaved] final.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/antidiabeticsautosavedfinal-231210163451-81c335f7-thumbnail.jpg?width=640&height=640&fit=bounds)























