The document discusses various topics related to anaesthesia including:
- Types of anaesthesia such as general, local and balanced anaesthesia.
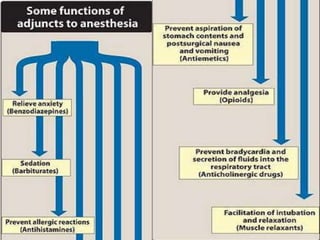
- Preanaesthetic medications that are used to relieve anxiety and prevent complications.
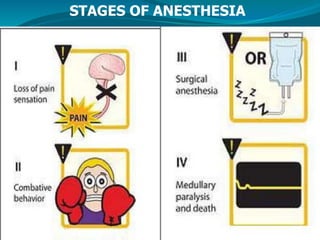
- Stages of anaesthesia from analgesia to medullary paralysis.
- Molecular targets of general anaesthetics such as GABA-A and NMDA receptors.
- Classification of anaesthetics into inhalational and intravenous agents.
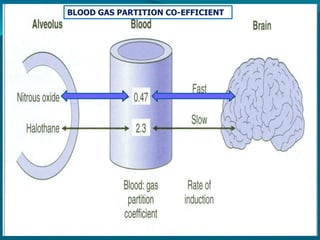
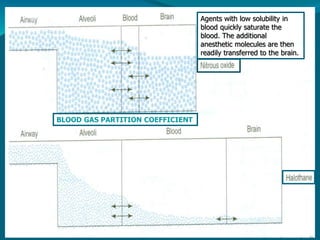
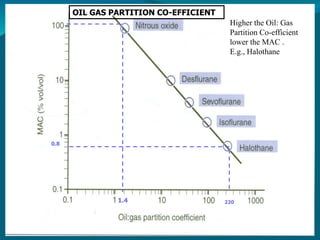
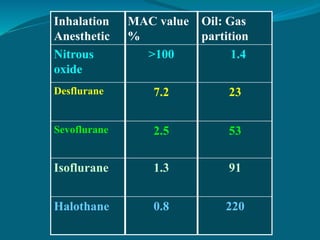
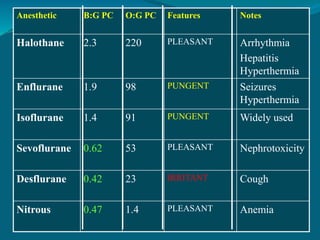
- Properties, uses and side effects of common inhalational agents like halothane, sevoflurane and nitrous oxide.
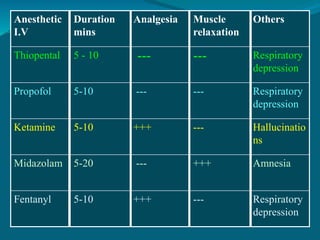
- Intravenous induction agents including thiopentone, propofol and ketamine.

























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


