Downloaded 20 times
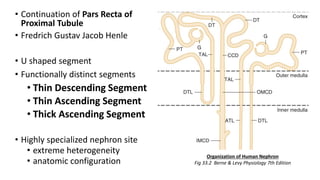
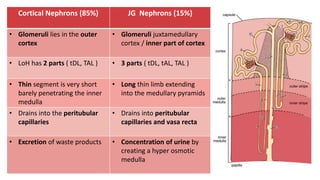
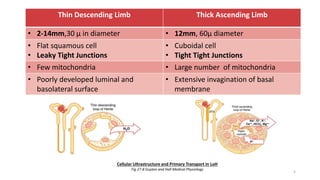
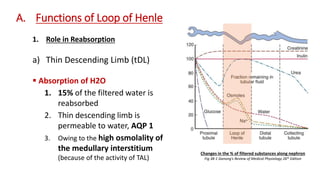
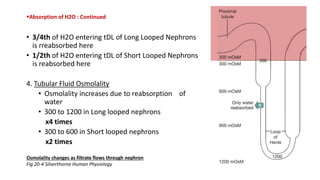
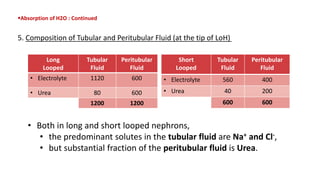
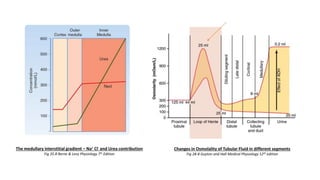


The document details the functions of the Loop of Henle, highlighting its role in reabsorption of water, concentration of urine, and acid-base balance. It describes the distinct characteristics and functions of the thin descending limb, thin ascending limb, and thick ascending limb, including ion transport mechanisms and their contributions to the renal medulla's osmotic gradient. Additionally, it discusses applied aspects such as the effects of loop diuretics and genetic disorders like Bartter syndrome.
































![Renal Physiology. [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/renalphysiology-250924082023-9109186b-thumbnail.jpg?width=640&height=640&fit=bounds)






















































