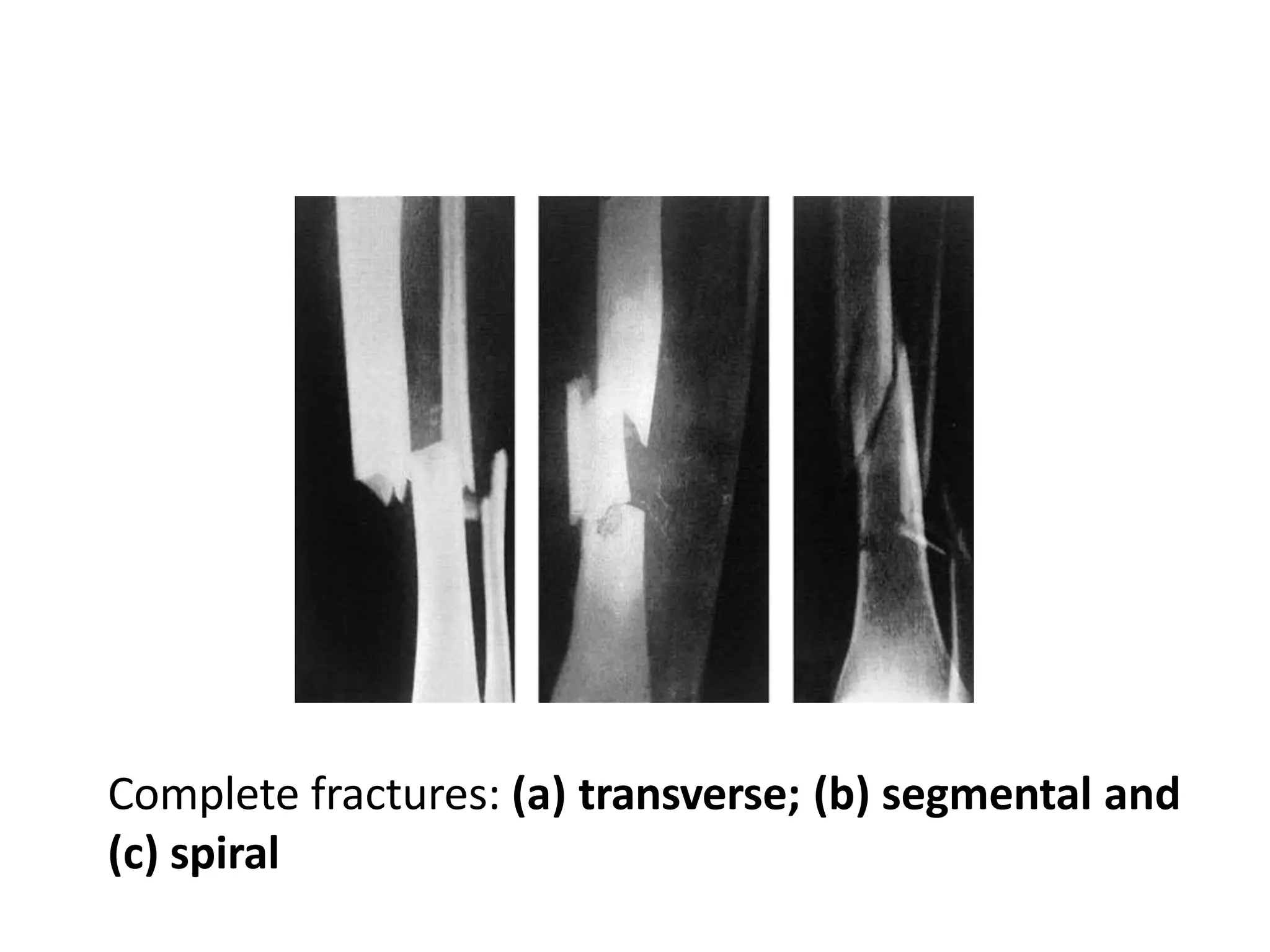
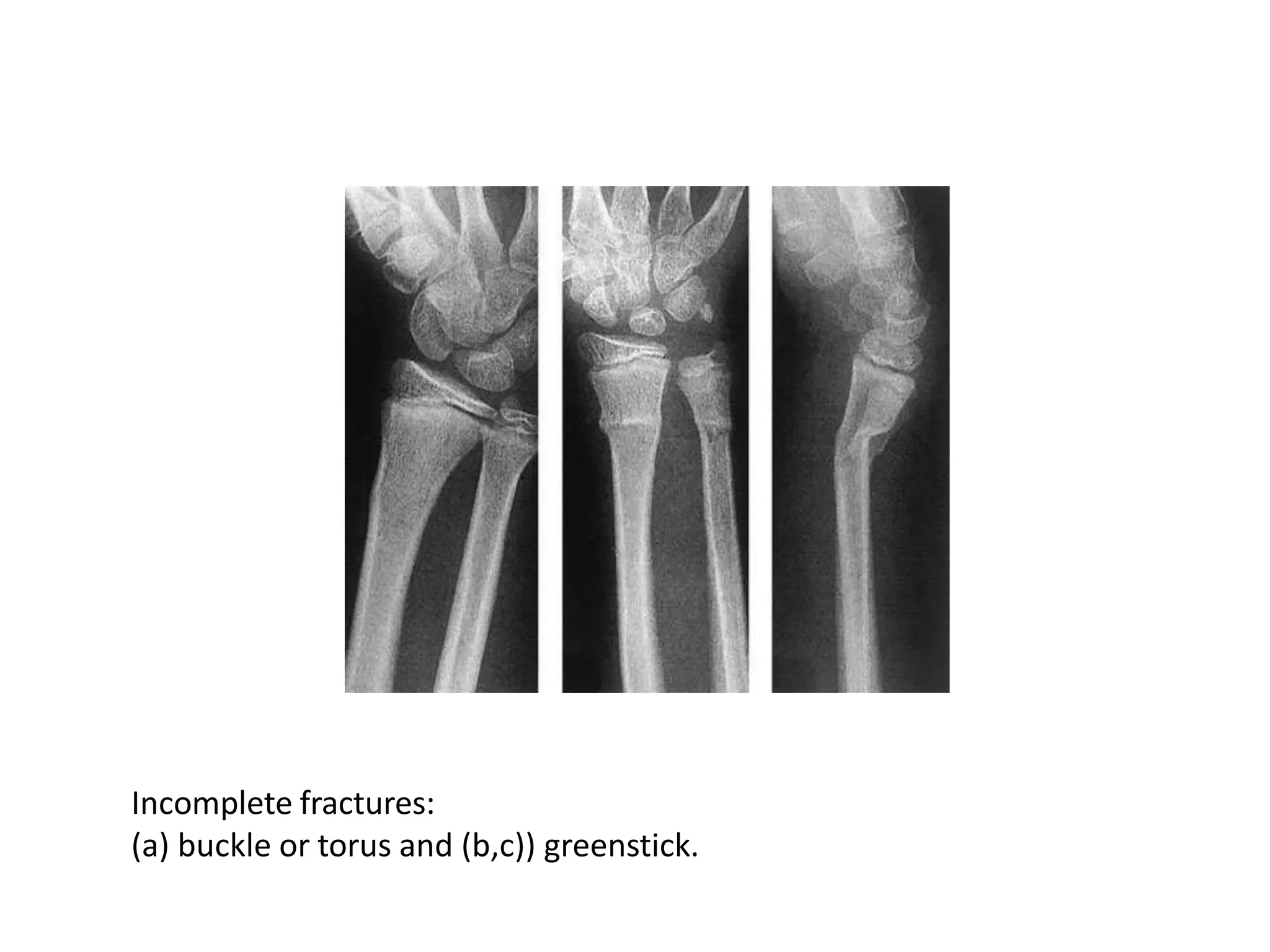
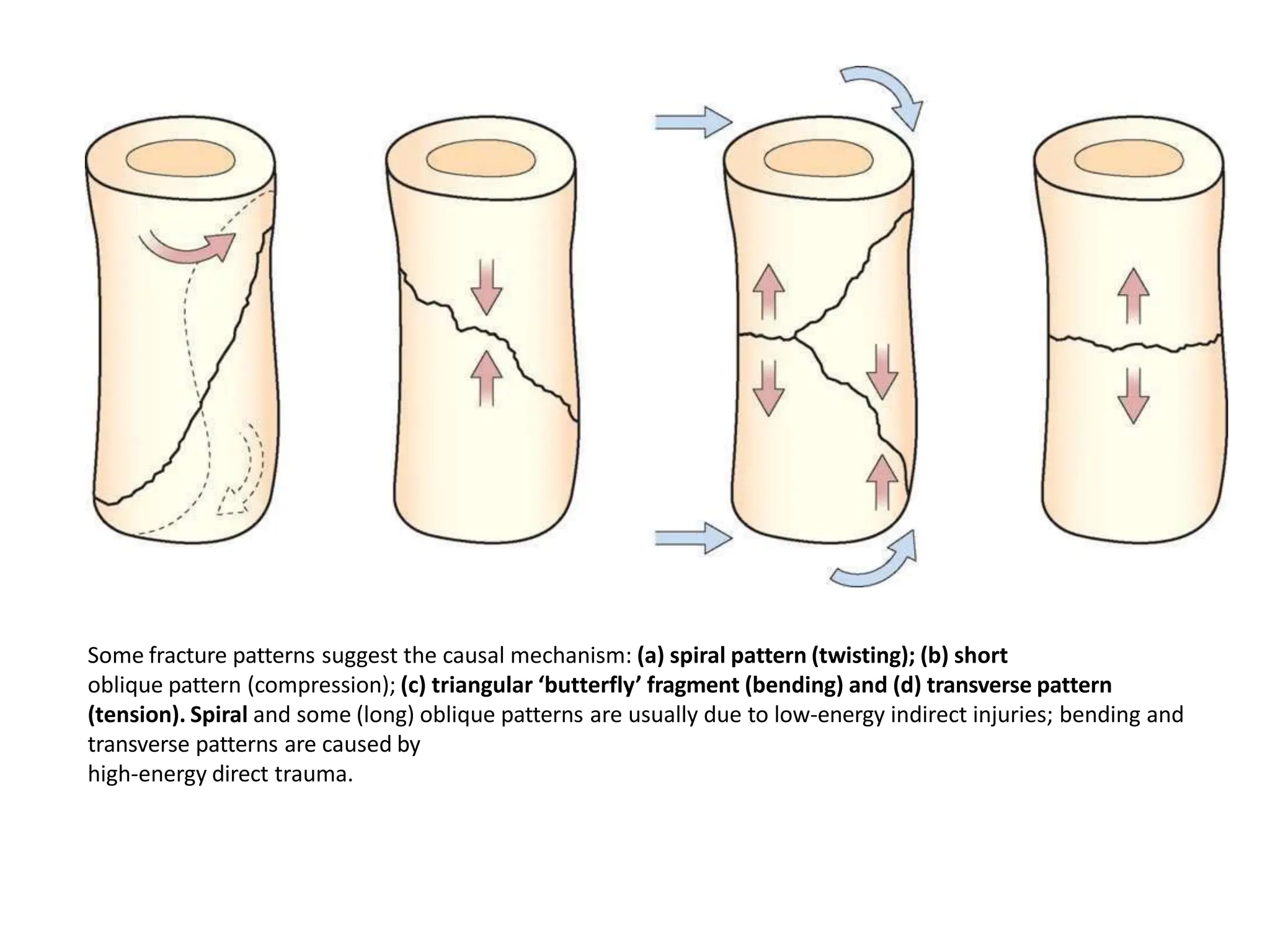
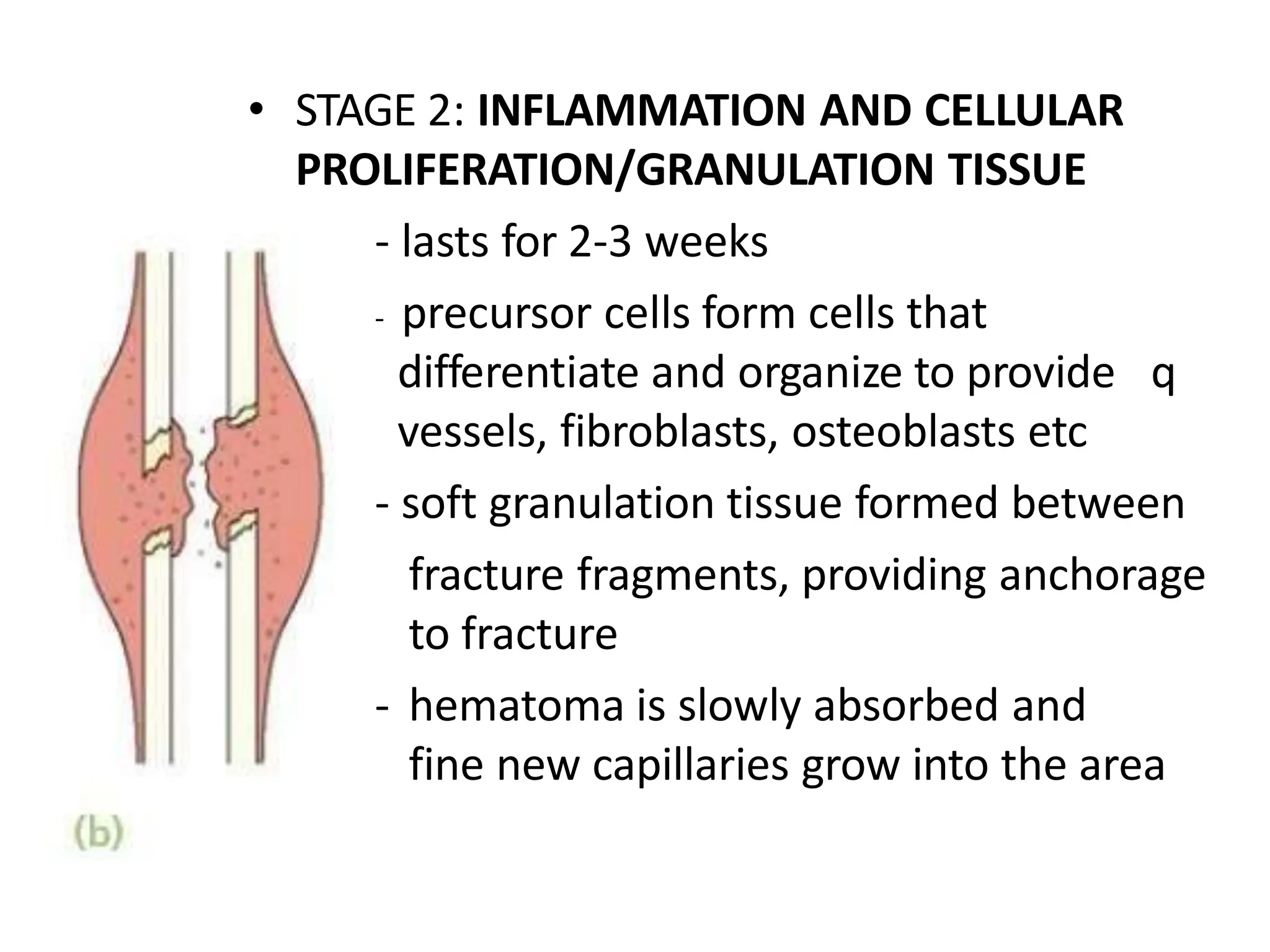
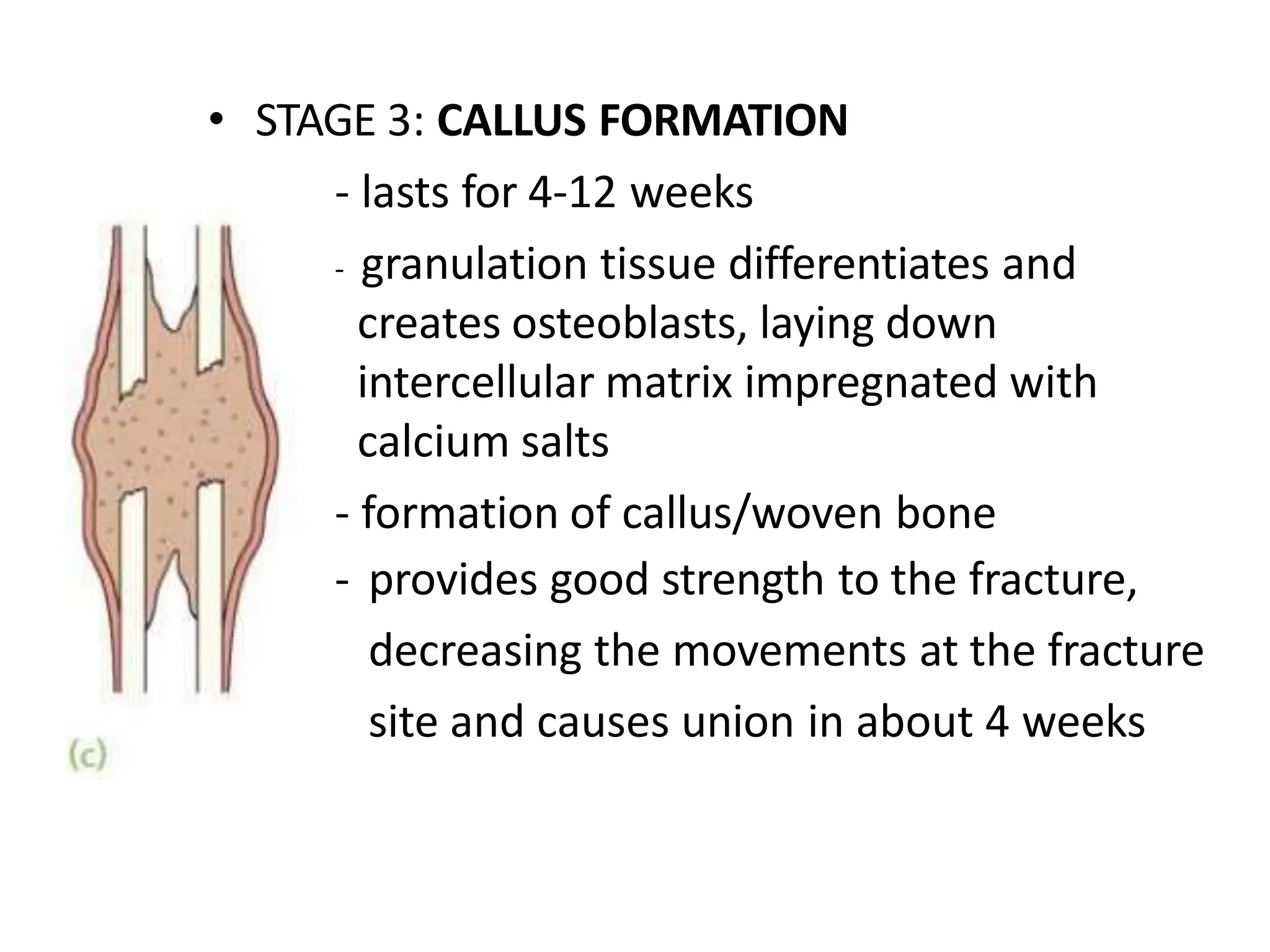
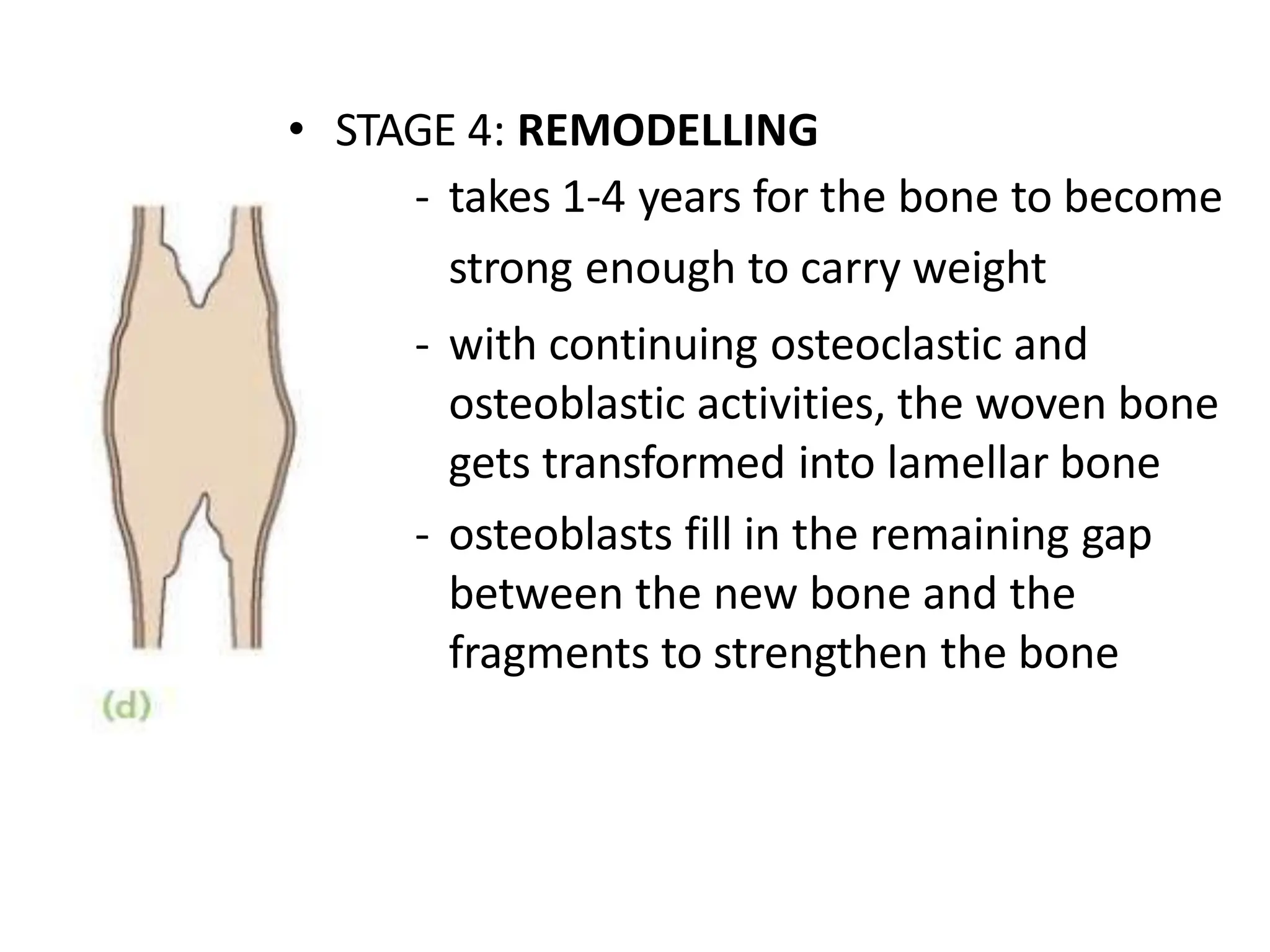
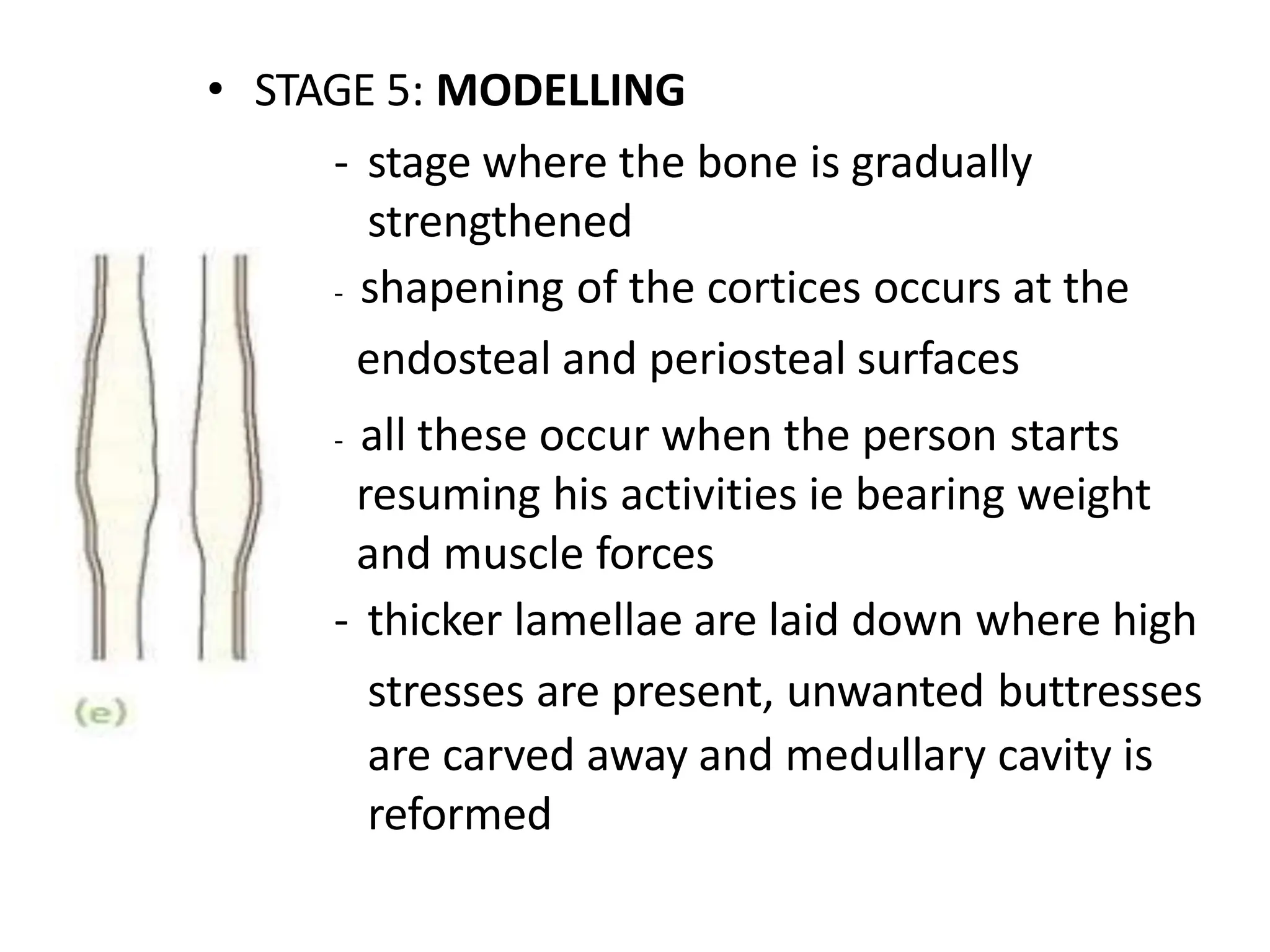
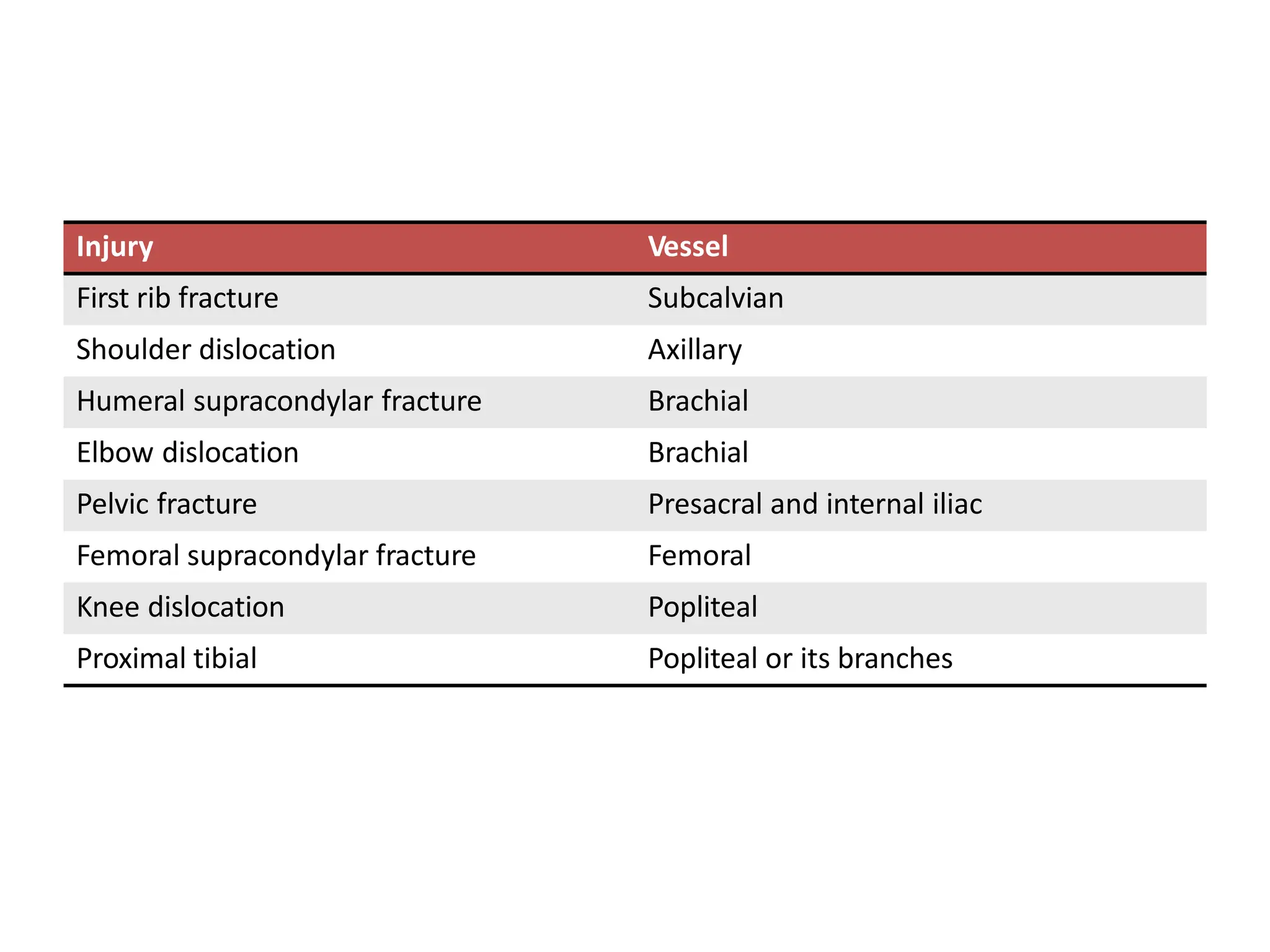
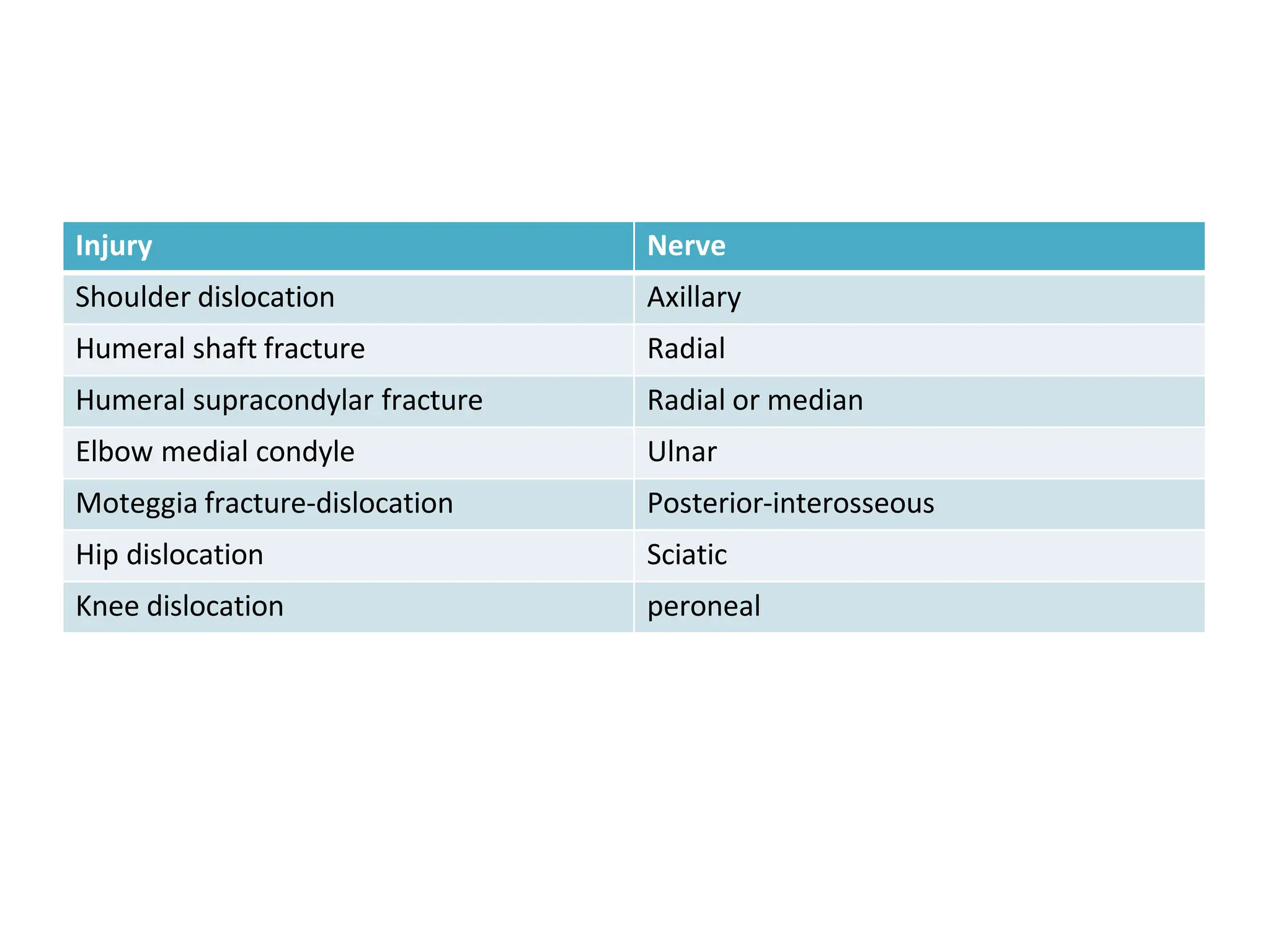
This document discusses fracture types, healing, complications, and treatment. It begins by defining fractures and classifying them as closed or open. Fractures are further divided into complete and incomplete types. Complete fractures result in two or more bone fragments, while incomplete fractures only partially divide the bone. Complications discussed include visceral injuries, vascular injuries which can result in impaired blood flow, and nerve injuries. Proper imaging including x-rays and additional imaging like CT or MRI is important for diagnosis. Factors that can affect bone healing and the stages of healing via callus formation or direct union are outlined. Clinical signs and symptoms are also reviewed.