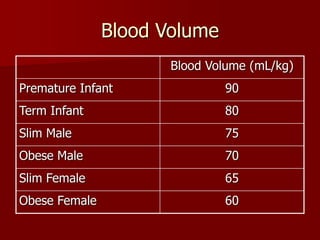
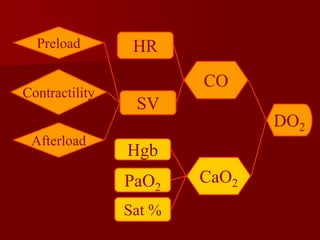
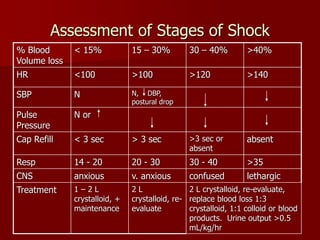
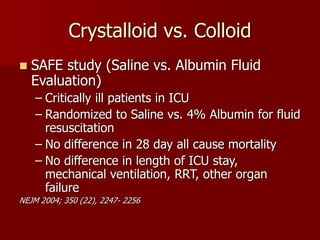
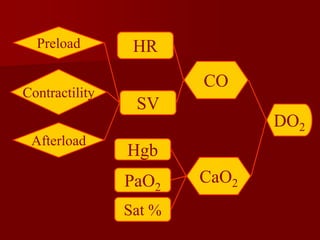
The document provides a comprehensive overview of fluid management and shock resuscitation, including fluid requirements, types of shock, and resuscitation goals. It details physiological fluid compartments, fluid deficit calculations, and various resuscitation fluids and their applications. Additionally, it discusses assessment methods for shock and fluid resuscitation strategies, emphasizing the importance of oxygen delivery to tissues.






















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













