Here are the procedures I would suggest based on the findings in each case:
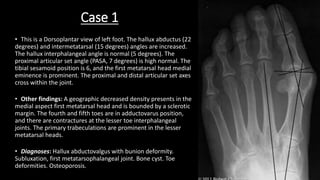
Case 1:
- Distal metatarsal osteotomy to decrease the intermetatarsal and hallux abductus angles and reduce the sesamoids.
- Possible cheilectomy or excision arthroplasty to address the bone cyst and osteoarthritis.
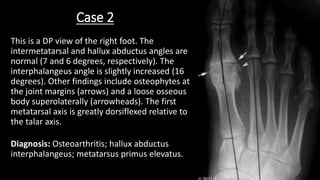
Case 2:
- Distal metatarsal osteotomy or proximal phalangeal osteotomy to address the increased interphalangeal angle and metatarsus primus elevatus.
- Possible cheilectomy to address the osteoarthritis.
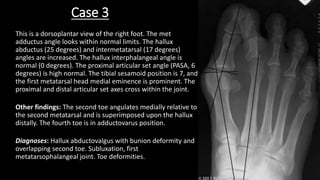
Case 3:
- Distal metatarsal osteotomy to decrease the intermetatarsal and hallux abduct