1. Talar fractures are usually the result of high-energy trauma and account for approximately 1% of all foot and ankle fractures.
2. The talus has a limited blood supply, so talar fractures can lead to avascular necrosis if not properly treated.
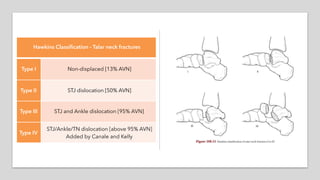
3. Fractures of the talar neck are the second most common type of talar fracture and are often classified using Hawkins' system from Type I to Type IV based on displacement and prognosis.

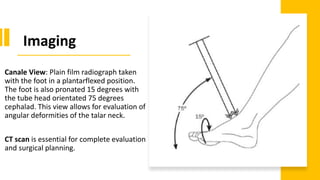
![Relevant
Anatomy
An intimate knowledge of the vascular supply
to the talus is essential with regard to
avascular necrosis (AVN):
[Aquino’s. Talar neck fractures: a review of
vascular supply and classification. J Foot Surg.
1986; 25(3): 188-93.]](https://image.slidesharecdn.com/talarfracture-200517214138/85/AJM-Sheet-Talar-fracture-6-320.jpg)
![Additional
Readings
Talar fractures are relatively uncommon in the
medical literature. Most studies are case
reports or small retrospective reviews leading
only to Level IV or V evidence.
[Ahmad J, Raikin SM. Current concepts review: talar fractures.
Foot Ankle Int. 2006 Jun; 27(6): 475-82.]
[Golano P, et al. The anatomy of the navicular and periarticular
structures. Foot Ankle Clin. 2004 Mar; 9(1): 1-23.]
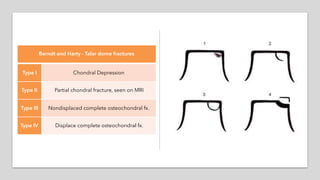
[Berndt A, Harty M. Transchondral fractures of the talus. JBJS-
Am. 1959; 41: 988-1020.]
[Canale ST, Kelly FB. Fractures of the neck of the talus. Long-term
evaluation of seventy-one cases. JBJS-Am. 1978 Mar; 60(2): 143-
56.]](https://image.slidesharecdn.com/talarfracture-200517214138/85/AJM-Sheet-Talar-fracture-21-320.jpg)






















































































