The document provides detailed information on calcaneal fractures, including epidemiology, classification systems, imaging, treatment approaches, and complications. Some key points:
- Intra-articular fractures account for approximately 75% of calcaneal fractures.
- Sanders classification is most commonly used, dividing fractures into 8 types based on number of fragments and location of fracture lines seen on CT scan.
- Goals of treatment are to restore calcaneal height, width, and alignment as well as achieve anatomic reduction of joints. Treatment may include closed reduction, ORIF, external fixation, or arthrodesis.
- Common complications include wound healing issues, post-traumatic arthritis, nerve damage, and mal



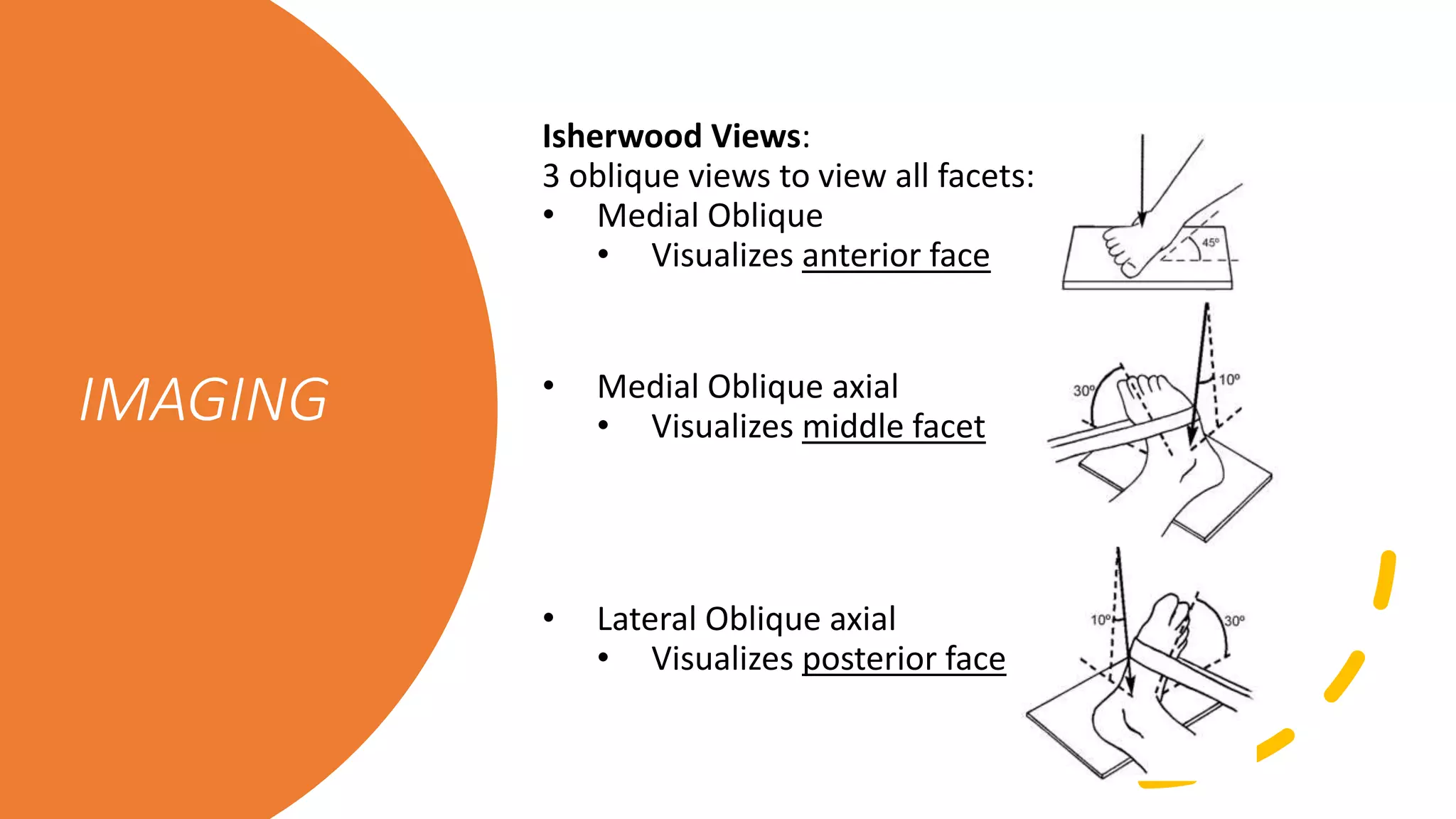
![IMAGING
• Bohler’s Angle: Normally 25-40 degrees.
[Decreased with fracture]
• Critical Angle of Gissane: Normally 125-140
degrees [Increased with fracture]](https://image.slidesharecdn.com/ajmsheet-calcanealfx-200517213957/75/AJM-Sheet-Calc-Fracture-7-2048.jpg)

![Sanders
Classification
Type “number” describes the # fragments formed
with fracture
A, B and C represent the location of fracture lines
A– Lateral
B – Center
C— Medial
Associated readings:
[Koval KJ, Sanders R. The radiographic evaluation of calcaneal fractures.
CORR. 1993 May; 290: 41-6.]
[Sanders R. Displaced intra-articular fractures of the calcaneus. JBJS-Am.
2000 Feb; 82(2): 225-50.]](https://image.slidesharecdn.com/ajmsheet-calcanealfx-200517213957/75/AJM-Sheet-Calc-Fracture-12-2048.jpg)


![Essex-Lopresti
Classification
Extra-articular (~25%)
Intra-articular (~75%)
• Tongue-type
• Joint depression
• fractures
Both intra-articular fractures
Have the same primary force, but different secondary
exit points.
[Essex-Lopresti P. The mechanism, reduction technique, and results in fractures of the os calcis.
Br J Surg 1952; 39: 395-419.]](https://image.slidesharecdn.com/ajmsheet-calcanealfx-200517213957/75/AJM-Sheet-Calc-Fracture-16-2048.jpg)
![Zwipp Classification
Assigns 2-12 points based
on:
• Number of fragments
• Number of involved
joints
• Open fracture or high
soft tissue injury
• Highly comminuted
nature, or associated
talar, cuboid, navicular
fractures [Rammelt S, Zwipp H. Calcaneus fractures: facts, controversies and
recent developments. Injury 2004; 35(5): 443-61.]](https://image.slidesharecdn.com/ajmsheet-calcanealfx-200517213957/75/AJM-Sheet-Calc-Fracture-17-2048.jpg)

![AJM Sheet:
Appreciate the debate in the literature
between cast immobilization vs.
percutaneous reduction vs. ORIF vs.
primary arthrodesis. Possible use of
delta frame to allow for closed reduction
and balancing of soft tissue swelling pre-
operatively.
[Barei DP, et al. Fractures of the calcaneus. Orthop Clin North Am. 2002 Jan;
33(1): 263-85.]
Review the lateral extensile surgical approach
[Benirschke SK, Sangeorzan BJ. Extensive intraarticular fractures of the foot. Surgical
management of calcaneal fractures. CORR. 1993 Jul; 292: 128-134.]](https://image.slidesharecdn.com/ajmsheet-calcanealfx-200517213957/75/AJM-Sheet-Calc-Fracture-19-2048.jpg)

![COMPLICATIONS
• Wound healing,
• Arthritis,
• Lateral ankle impingement,
• Malunion,
• Non-union, etc.
[Benirschke SK, Kramer PA. Wound healing complication in closed and open calc fractures. J
Orthop Trauma. 2004; 18(1): 1-6.]
[Cavadas PC, Landin L. Management of soft-tissue complications of the lateral approach for
calcaneal fractures. Plast Reconstr Surg. 2007; 120(2): 459-466.]](https://image.slidesharecdn.com/ajmsheet-calcanealfx-200517213957/75/AJM-Sheet-Calc-Fracture-21-2048.jpg)