
























![DRUG INTERACTIONS WITH EPINEPHRINE AND
LEVONORDEFRIN
Nonselective ß-blockers-
Tricyclic antidepressants-
General anesthetic (halothane ,
Fluothane] serious cardiac
dysrhythmia
Cocaine
So, FELYPRESSIN SAFER. 33](https://image.slidesharecdn.com/finallapptkhush-200302060630/75/Final-la-ppt-khush-33-2048.jpg)







































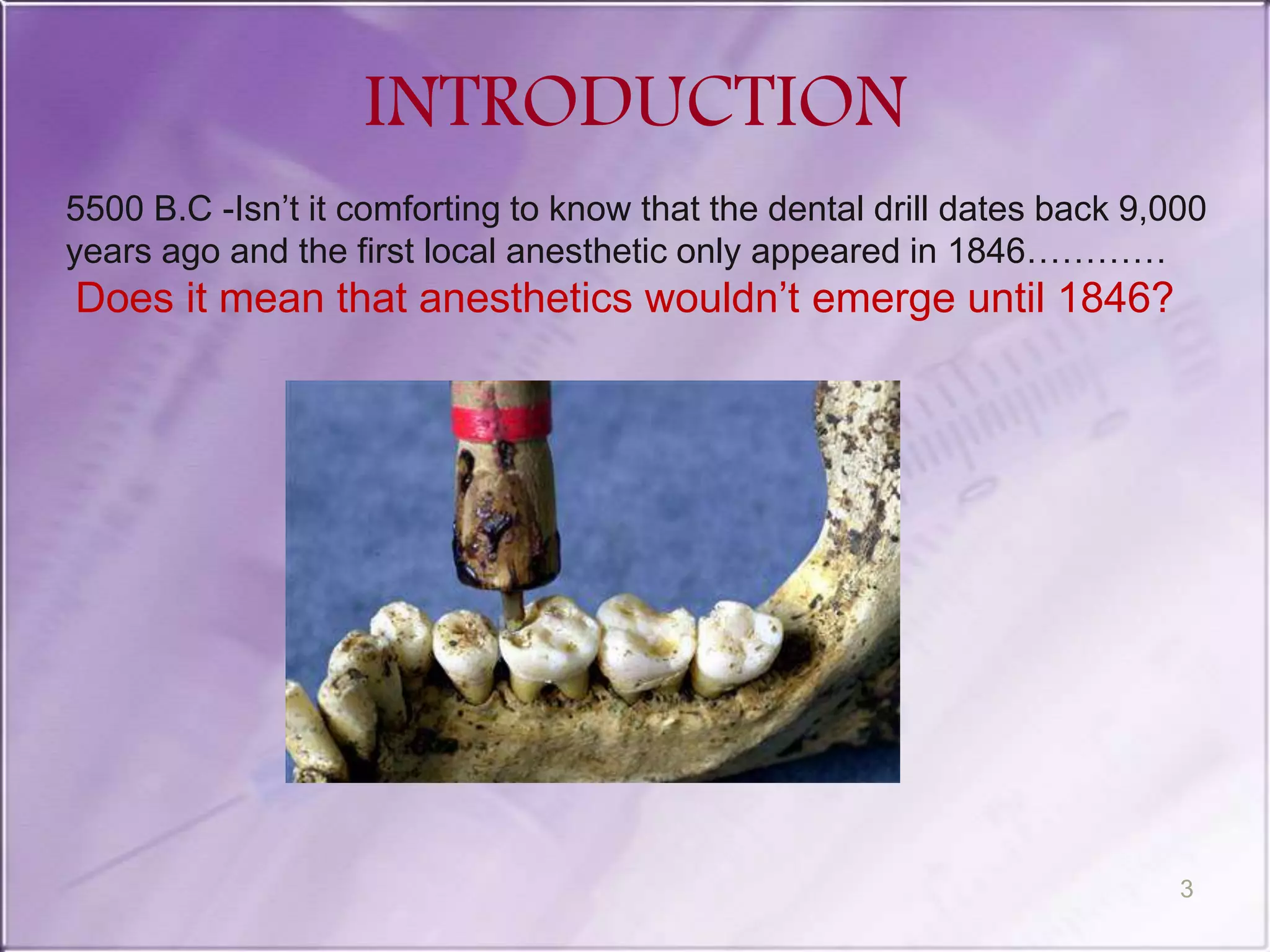
The document provides information on local anesthetics used in dentistry. It begins with definitions of local anesthesia and local anesthetic agents. It then discusses the history of local anesthesia, ideal properties, mechanism of action, pharmacokinetics, commonly used local anesthetic drugs (lidocaine, bupivacaine, articaine), dosages, and complications. It also covers topics like vasoconstrictors, topical anesthetics, and recent advances in local anesthesia.








































![10. Local anaesthetics [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/10-230227080146-90018189-thumbnail.jpg?width=640&height=640&fit=bounds)




























![Understanding Parkinson’s Disease: Causes, Symptoms, and Treatment [2025]](https://cdn.slidesharecdn.com/ss_thumbnails/understandingparkinson-251208102525-80ba3223-thumbnail.jpg?width=640&height=640&fit=bounds)

















