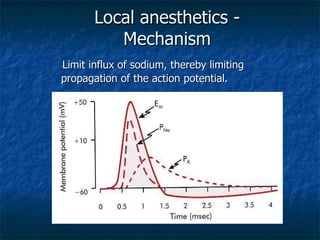
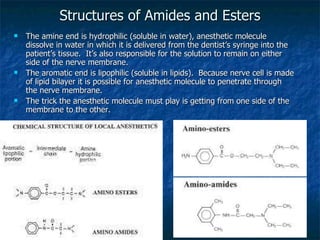
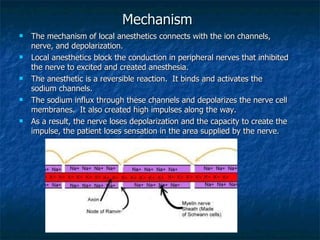
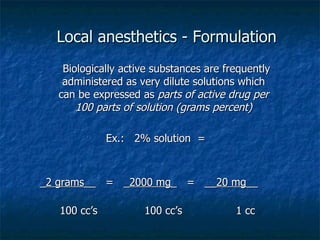
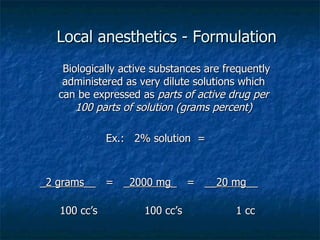
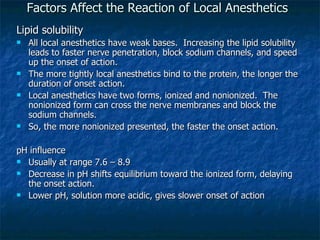
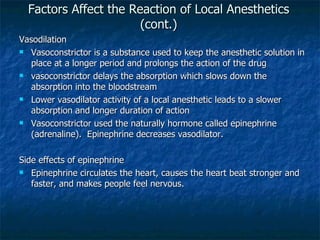
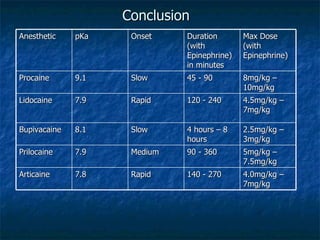
Local anesthetics work by blocking sodium channels in nerves, limiting the propagation of action potentials and producing loss of sensation in a specific area. Early local anesthetics like cocaine and procaine had limitations. Lidocaine, introduced in 1940, was a major breakthrough as the first modern local anesthetic due to its quick onset of action, duration of several hours, and minimal allergenicity. The two classes of local anesthetics are esters and amides; amides are preferable due to lower risk of allergic reactions. Factors like lipid solubility, pH, vasoconstrictors, and dosage levels affect the onset and duration of local anesthetics.














































![lec 14 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/lec14autosaved-230315142106-831cdef1-thumbnail.jpg?width=640&height=640&fit=bounds)
![10. Local anaesthetics [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/10-230227080146-90018189-thumbnail.jpg?width=640&height=640&fit=bounds)

















![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







