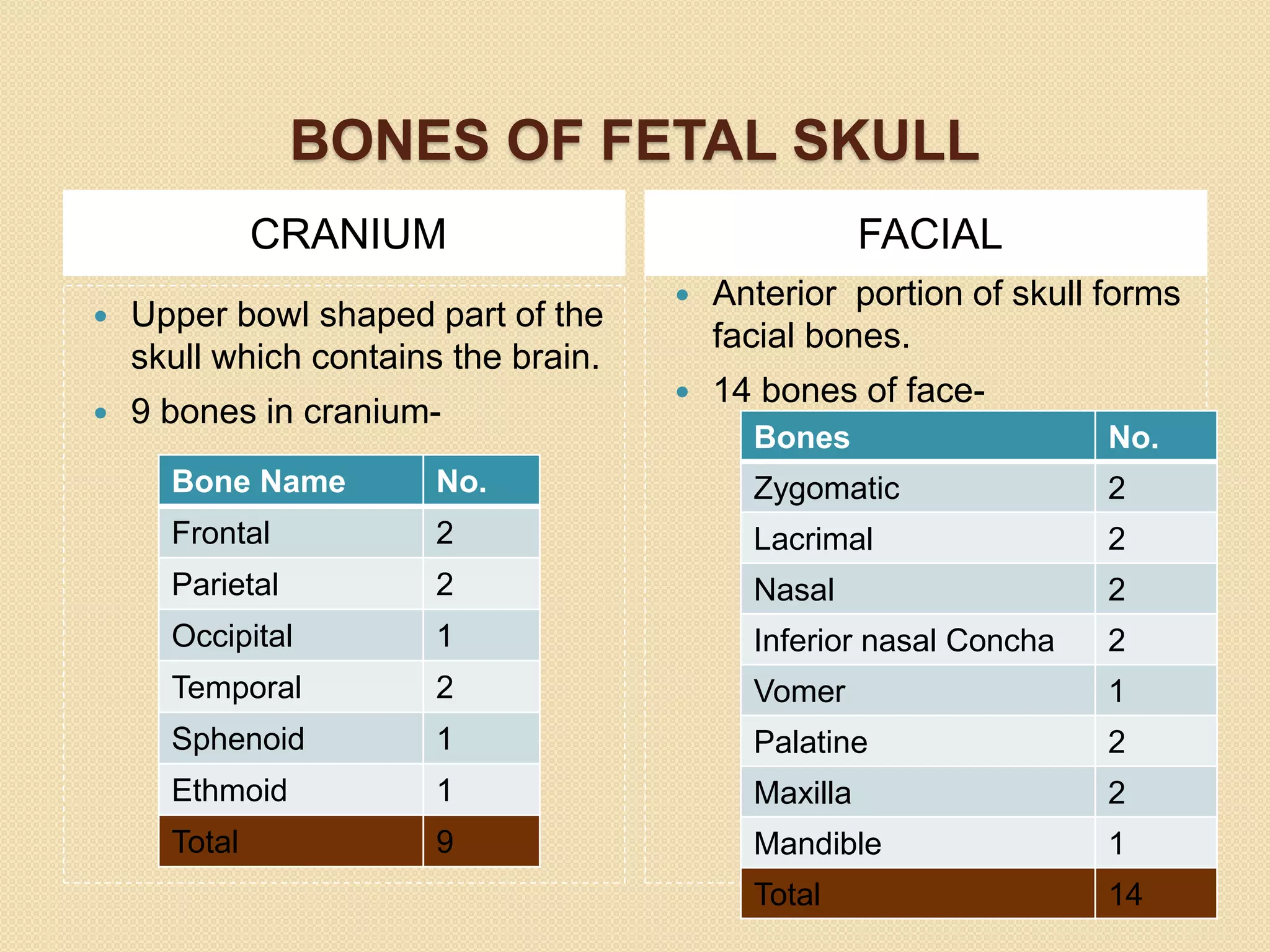
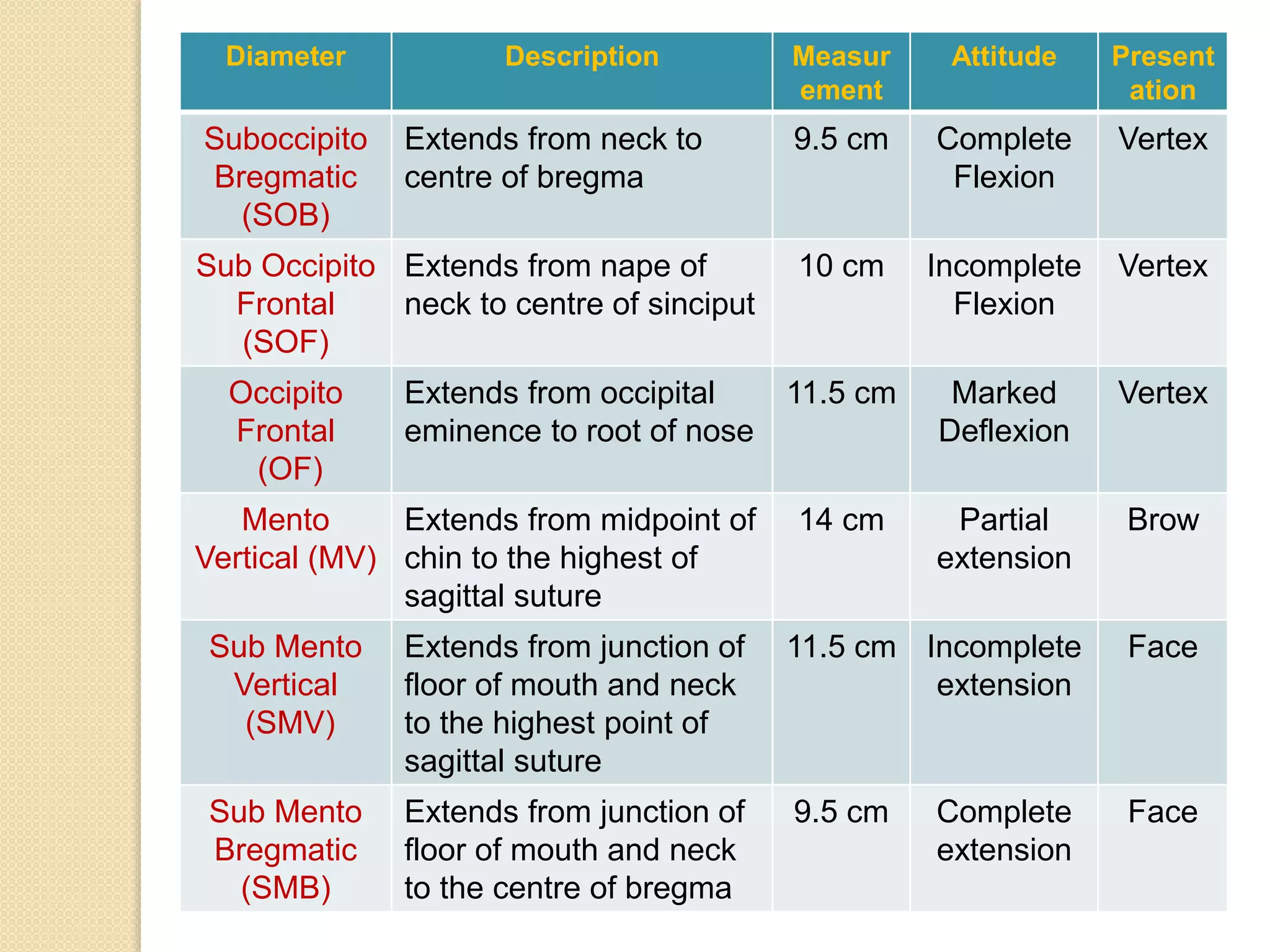
The document discusses the significance of the fetal skull in obstetrics, highlighting its function in protecting vital organs and being the first part that enters the birth canal during delivery. It details the anatomy of the skull, including its bones, sutures, fontanelles, and relevant diameters, as well as their clinical importance during labor. A midwife's understanding of these elements is crucial for assessing the fetus's position and ensuring a smooth delivery.