
Recommended
Recommended
More Related Content
What's hot
What's hot (20)
Similar to FETAL SKULL DISCUSSION (1).pdf
Similar to FETAL SKULL DISCUSSION (1).pdf (20)
More from Komal Upreti
Recently uploaded
Recently uploaded (20)
FETAL SKULL DISCUSSION (1).pdf
- 1. 1 RAJKUMARI AMRIT KAUR COLLEGE OF NURSING LAJPAT NAGAR, NEW DELHI MATERIAL ON DISCUSSION OF FETAL SKULL SUBJECT: OBSTETRICS AND GYANECOLOGICAL NURSING TOPIC: FETAL SKULL DATE OF SUBMISSION : 22nd AUGUST 2023 SUBMITTED TO: SUBMITTED BY: Mrs. ANUGRAH MILTON Ms. KOMAL UPRETI HEAD OF DEPARTMENT M.Sc. NURSING OBSTETRICS & GYNAECOLOGICAL NURSING FIRST YEAR RAK COLLEGE OF NURSING
- 2. 2 FETAL SKULL INTRODUCTION Understanding the anatomy of the fetal skull and its diameter will help us recognise how a labour is progressing, and whether the baby's head is 'presenting' correctly as it comes down the birth canal. This will give you a better understanding of whether a normal vaginal delivery is likely, or if the mother needs referral because the descent of the baby's head is not & making sufficient progress. The fetal head is large in relation to the fetal body compared with the adult. The fetal skull is the most difficult part of the baby to pass through the mother's pelvic canal, due to the hard bony nature of the skull. Adaptation between the fetal skull and the pelvis is necessary to allow the head to pass through the pelvis during labour without complications. OBJECTIVES Define the fetal skull. Enumerate the importance of fetal skull. Describe the divisions and regions of the fetal skull. Enlist the bones which constitute the fetal head. Elaborate the sutures and fontanelles in fetal skull and their importance. Describe the various diameters and circumferences of the fetal skull and their significance. Discuss the moulding and its relevance. Identify types of injury that can occur to the fetal skull during labour and birth. DEFINITION OF FETAL SKULL Figure 1 FETAL SKULL Fetal skull is the part of fetal body which encase and protect the brain. Skull is compressible to some extent because it made up of thin flat bones which forms the vault. This is anchored to the rigid and incompressible bones at the base of the skull. FIG 1: FETAL SKULL
- 3. 3 IMPORTANCE OF FETAL SKULL 1. Largest part of the fetal body. 2. Most frequent presenting part of the fetus during delivery. 3. Least compressible among all the fetal parts. DIVISONS OF FETAL SKULL The fetal skull has divided into 3 major parts: o Vault o Base o Face Fig 2 : Fetal skull showing different regions VAULT: The vault is the large, dome-shaped part above an imaginary line drawn between the orbital ridges and the nape of the neck. BASE: The base comprises bones that are firmly united to protect the vital centres in the medulla oblongata. FACE: The face is composed of 14 small bones that are also firmly united and non-compressible.
- 4. 4 REGIONS OF FETAL SKULL The fetal skull has divided into different regions which are of obstetrical importance: o Vertex o Brow o Face o Sinciput o Occiput VERTEX It is a quadrangular area bounded anteriorly by the bregma and coronal sutures behind the lambda and lambdoid sutures and laterally by lines passing through the parietal eminences. BROW It is an area bounded on one side by the anterior fontanelle and coronal sutures and on the other side by the root of the nose and the supra orbital ridges of the either side. The base comprises bones that are firmly united to protect the vital centres in the medulla oblongata. FACE It is the area bounded on one side by root of the nose and supra orbital ridges and on the other, by the junction of the floor of the mouth and neck. The point between the eyebrows is known as glabella. SINCIPUT It is the area lying in front of the anterior fontanelle and corresponds to the area of brow. OCCIPUT It is the area limited to the occipital lobe.
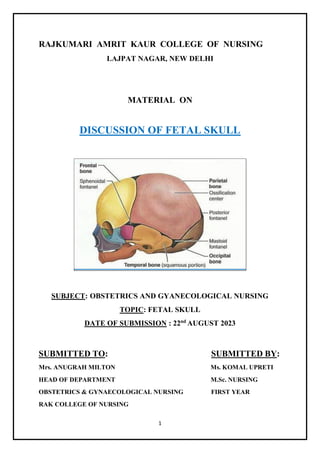
- 5. 5 Fig 3 : Fetal skull showing different regions and landmarks of obstetrical significance BONES OF FETAL HEAD Fetal head is consists of 7 bones: 2 frontal bone 2 parietal bone 2 temporal bone 1 occipital bone Fig 4 : Bones of fetal head
- 6. 6 SUTURES AND FONTANELLES Flat bones of the vault are united together by non-ossified membranes attached to the margins of the bones , these are called sutures and fontanelles. These sutures and fontanelles are of obstetric significance because they allow moulding of the fetal head during labour. SUTURES: Four types of sutures are found in the fetal skull:- 1. Sagittal or longitudinal suture: Lies between two parietal bones. 2. Coronal suture: Between parietal and frontal bones on either side. 3. Frontal suture: Lies between two frontal bones. 4. Lambdoid suture: Separate the occipital bone and the two parietal bones. Fig 5 : Image showing the sutures and fontanelles IMPORTANCE OF SUTURES: (a) It permits gliding movement of one bone over the other during moulding of the head, a phenomenon of significance while the head passes through the pelvis during labour. (b) Digital palpation of sagittal suture during internal examination in labour gives an idea of the manner of engagement of the head, degree of internal rotation of the head and degree of moulding of the head.
- 7. 7 FONTANELLES: Wide gap in the suture line is called fontanelle. There are six fontanelles in number but out of these six only two are of obstetrics significance. 1. Posterior fontanelle 2. Anterior fontanelle POSTERIOR FONTANELLE The posterior fontanelle or lambda is situated at the junction of the lambdoidal and sagittal sutures. It is small, triangular in shape and can be recognized vaginally because a suture leaves from each of the three angles. It normally closes by 6 weeks of age. Fig 6: Image showing anterior and posterior fontanelle ANTERIOR FONTANELLE The anterior fontanelle or bregma is found at the junction of the sagittal, coronal and frontal sutures.
- 8. 8 It is broad, kite or diamond shaped and recognizable vaginally because a suture leaves from each of the four corners. It measures 3–4 cm long and 1.5–2 cm wide and normally closes by 18 months of age. Pulsations of cerebral vessels can be felt through this fontanelle. IMPORTANCE OF FONTANELLES: (a) Its palpation through internal examination denotes the degree of flexion of the head. (b) It facilitates moulding of the head. (c) As it remains membranous long after birth, it helps in accommodating the marked brain growth; the brain becoming almost double its size during the first year of life. (d) Palpation of the floor reflects intracranial status: depressed in dehydration, elevated in raised intracranial tension. (e) Collection of blood and exchange transfusion, on rare occasion, can be performed through it via the superior longitudinal sinus. (f) Cerebrospinal fluid can be drawn, although rarely, through the angle of the anterior fontanel from the lateral ventricle. (g) Denotes the position of head in relation to maternal pelvis. DIAMETERS OF SKULL The engaging diameter of the fetal skull depends on the degree of flexion present. According to measurement whole skull is divided into two i.e. Anterior posterior diameter Transverse diameter.
- 9. 9 1. ANTERIOR POSTERIOR DIAMETER Fig 7 : Anterior posterior diameters of the fetal head (a) Suboccipito bregmatic (SOB) Extends from the nape of the neck to the centre of the bregma. 9.5cm in diameter. Attitude of the head is Complete flexion. Presentation is Vertex. (b) Sub-occipitofrontal (SOF) Extends from the nape of the neck to the anterior end of the anterior fontanelle or the centre of the sinciput. 10cm in diameter. Attitude of the head is Incomplete flexion. Presentation is Vertex. (c) Occipitofrontal (OF) Measured from the occipital eminence to the glabella.
- 10. 10 11.5cm in diameter. Attitude of the head is Marked deflexion. Presentation is Vertex. (d) Mento vertical (MV) Measured from the point of the chin to the highest point on the sagittal suture. 14cm in diameter. Attitude of the head is Partial extension. Presentation is Brow. (e) Sub-mento vertical (SMV) Measured from the point where the chin joins the neck to the highest point on the vertex. 11.5cm in diameter. Attitude of the head is Incomplete extension. Presentation is Face. (f) Sub-mento bregmatic (SMB) Measured from the point where the chin joins the neck to the centre of the bregma. 9.5cm in diameter. Attitude of the head is Complete extension. Presentation is Face. Fig 8: Image showing measurement of anterior posterior diameter
- 11. 11 2. TRANSVERSE DIAMETER Fig 9 :Transverse diameter of fetal head (a)Biparietal diameter Extends between two parietal eminences. Whatever may be the position of the head, the diameter nearly always engages. 9.5cm in diameter. (b)Bitemporal diameter It is the distance between the antero-inferior ends of the coronal suture. 8.2cm in diameter. (c) Super- subparietal diameter It extends from a point placed below one parietal eminence to a point placed above the other parietal eminence of the opposite side. 8.5cm in diameter. (d)Bimastoid diameter It is the distance between the tips of mastoid process. 7.5cm in diameter.
- 12. 12 CIRCUMFERENCES: Circumference of the plane of the diameter of engagement differs according to the attitude of the head. ATTITUDE OF THE HEAD PLANE OF ENGAGEMENT SHAPE CIRCUMFERENCE Complete Flexion Biparietal sub occpito bregmatic Almost round 27.5cm Deflexed Biparietal sub occpito frontal Oval 34cm Incomplete extension Biparietal mento vertical Bigger oval 37.5cm Complete extension Biparietal sub mento bregmatic Almost round 27.5cm MOULDING The overlapping of the fetal skull bones at the suture line. (Wylie, 2005, p.201) Bones of vault allow slight bending and override one another at the sutures. Skull changes shape from ovoid to cylindrical. Causes presenting diameter to decrease while increasing the diameter at right angles. It is the alteration of the shape of the fore-coming head while passing through the resistant birth passage during labour. (D C Dutta,2013,p.86) MECHANISM OF MOULDING: There is compression of the engaging diameter of the head with corresponding elongation of the diameter at right angle to it.
- 13. 13 Thus, in well flexed head of the anterior vertex presentation, the engaging suboccipito bregmatic diameter is compressed with elongation of the head in mento-vertical diameter which is at right angle to suboccipito bregmatic. Moulding disappear within few hours after birth. GRADING: There are three gradings:- Grade-1—the bones touching but not overlapping. Grade-2— overlapping but easily separated. Grade-3—fixed overlapping. IMPORTANCE OF MOULDING: Slight moulding is good and beneficial because it enables the head to pass more easily, through the birth canal. Shape of the moulding can be a useful information about the position of the head occupied in the pelvis. INJURIES DURING THE DELIVERY OF HEAD Fig 10: image showing caput succedaneum CAPUT SUCCEDANEUM Oedematous swelling that occurs on the presenting part. Present at birth. Can cross over the sutures. Soft swelling and will indent with pressure. Decreases following delivery. No treatment is required. Will disappear approximately 24-48hrs after birth. Moulding will also be apparent.
- 14. 14 Fig 11: Image showing cephalohematoma CEPHALOHEMATOMA Bleeding that occurs between the bones of the fetal skull and periosteum. Occurs 12-72 hours after birth. The swelling is restricted to one area and will not indent with pressure. Does not cross over the sutures. Can be bilateral. Persist for a few weeks and occasionally months.
- 15. 15 BIBLIOGRAPHY Burden, B. and Sapsed, M.S., The Fetal Skull. In: Macdonald, S.,Magill- Cuerden (eds.) Mayes' Midwifery 14th ed. London: Ballière Tindall, 2011, page no: 96-104. Wylie, L., Essential anatomy and physiology in maternity care. 2nd ed. Edinburgh: Elsevier,2005,page no: 201-206. Shirish S Sheth, Essential of Obstetrics, 1st Edition, Jaypee Brothers Medical Publishers, New Delhi,2004, page no.: 102 - 104. Diane M, Myles Textbook for Midwives, 14th edition, Elsevier Publisher, London, 2008, page no: 118-123. Dutta D C, Textbook of obstetrics,7th edition, New central book agency (P) ltd. ,London ,2013, page no: 83-87. Shirish N Daftary, Manual of obstetrics,2nd edition, Elsevier publication, 2007, Page no: 68-72. REFERENCES FOR THE IMAGES IMAGES REFERENCE Figure 1 & 2 https://www.google.com>fetalskull// Figure 3 & 9 Dutta D C, Textbook of obstetrics,7th edition, New central book agency (P) ltd. ,London ,2013, page no: 83-87. Figure 4 Diane M, Myles Textbook for Midwives, 14th edition, Elsevier Publisher, London, 2008, page no: 118-123. Figure 5 & 6 Wylie, L., Essential anatomy and physiology in maternity care. 2nd ed. Edinburgh: Elsevier,2005,page no: 201-206. Figure 7 & 8 Shirish N Daftary, Manual of obstetrics,2nd edition, Elsevier publication, 2007, Page no: 68-72.
- 16. 16 Figure 10 & 11 Burden, B. and Sapsed, M.S.,The FetalSkull.In:Macdonald,S.,Magill- Cuerden (eds.) Mayes' Midwifery 14th ed. London: Ballière Tindall, 2011, page no: