Downloaded 83 times
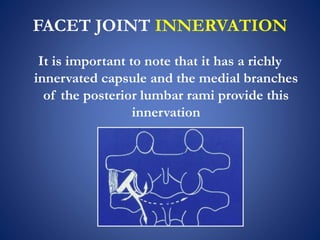
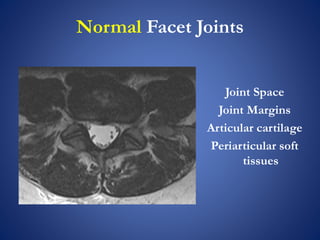
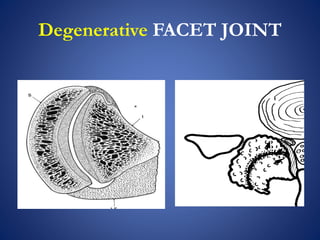
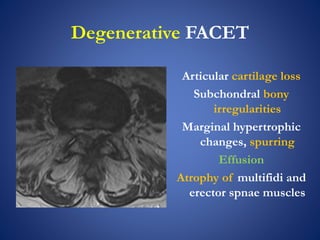
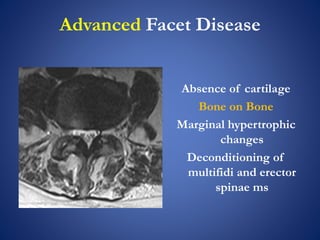
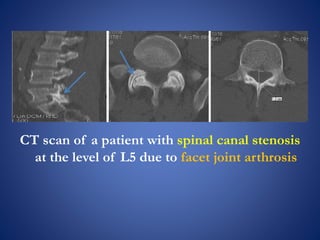
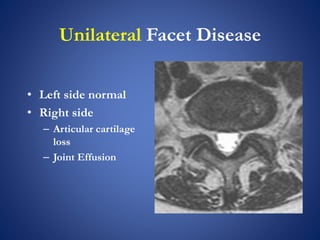
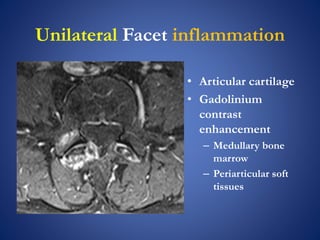
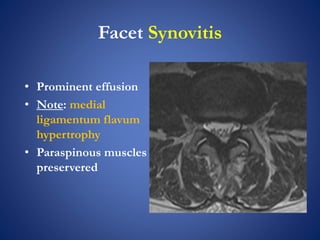

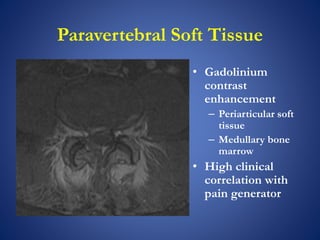
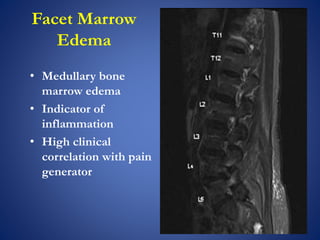
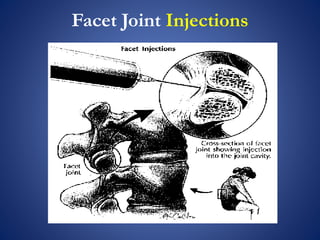
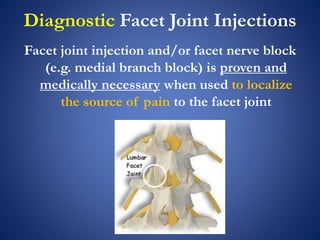

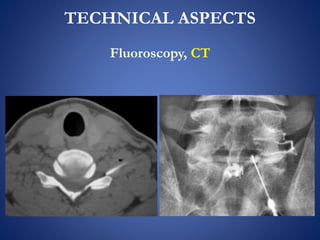
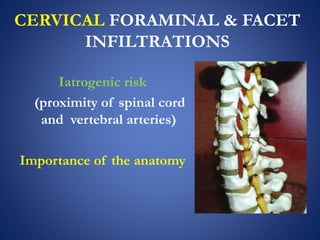
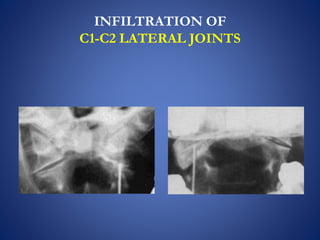
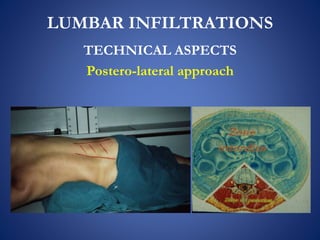
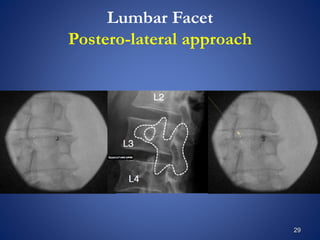
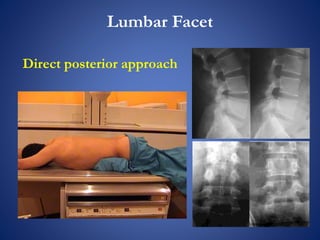
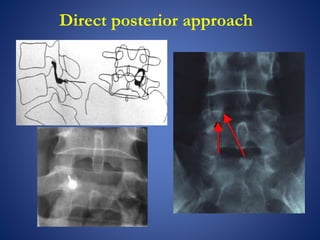


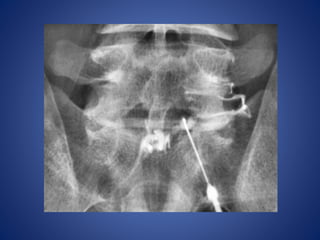

This document discusses facet joint injections for treating back pain. It describes the innervation and anatomy of normal and degenerative facet joints. Facet joint injections involve injecting local anesthetics and/or steroids into or near the facet joint under fluoroscopy or CT guidance. They can be used diagnostically to determine if facet joints are a source of pain or therapeutically to reduce inflammation and pain. The techniques for cervical, lumbar, and C1-C2 injections are covered, along with important technical aspects and potential complications. While facet joint injections are commonly used to treat facetogenic back pain, more research is still needed to evaluate their long-term effectiveness.























































































