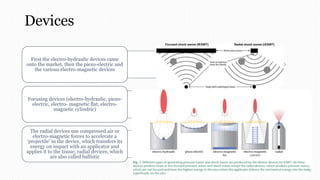
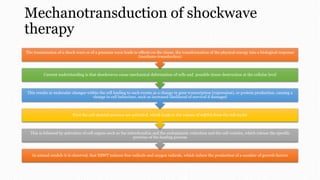
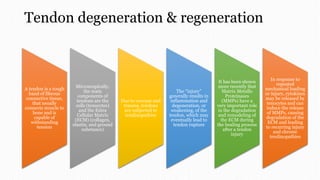
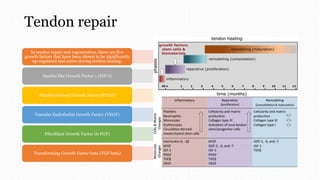
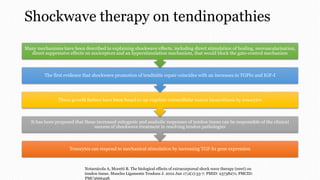
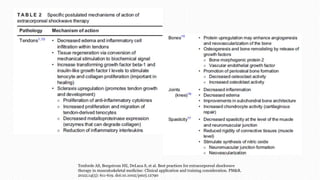
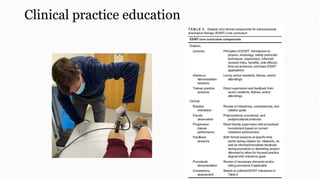
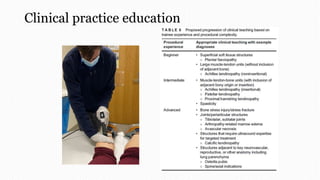
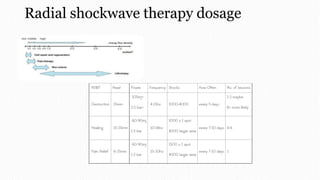
ESWT involves using shockwaves to treat various musculoskeletal conditions. There are two main types of ESWT - focused and radial. Focused ESWT uses higher pressure shockwaves that can penetrate deeper, while radial ESWT uses lower pressure shockwaves that spread out radially. ESWT stimulates the release of growth factors that promote tissue healing at the cellular level by activating mechanisms like increased gene expression and protein production. It has shown effectiveness in treating tendinopathies by up-regulating growth factors involved in tendon repair and regeneration. Proper clinical application and dosage depend on the device and condition being treated.





















![Avulsion fractures ppt [1]](https://cdn.slidesharecdn.com/ss_thumbnails/avulsionfracturespptashleyandsarahmusculo1-101129093116-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)














![Lect 9 (shock wave)[1]FHJ;LMOMXMOALANlad](https://cdn.slidesharecdn.com/ss_thumbnails/lect9shockwave1-251217213108-dfa314ce-thumbnail.jpg?width=640&height=640&fit=bounds)









![Shockwave [Read-Only].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/shockwaveread-only-220729144108-2f959010-thumbnail.jpg?width=640&height=640&fit=bounds)










































