Downloaded 19 times
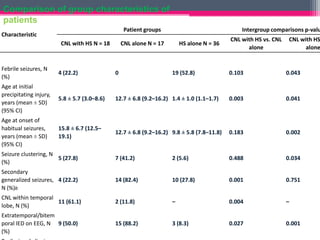
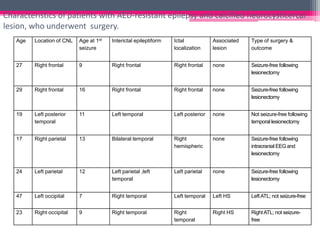
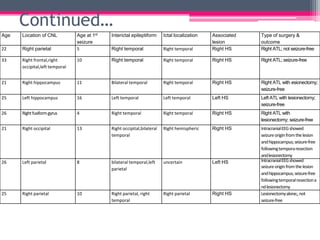
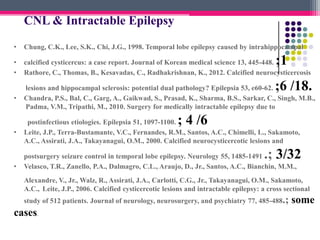

This study assessed the association between calcified neurocysticercosis lesions (CNLs) and antiepileptic drug-resistant epilepsy through a prospective analysis of 45 patients in South India with CNLs. The study divided patients into three groups: CNL alone (n=17), CNL with unilateral hippocampal sclerosis (HS) (n=18), and CNLs as incidental findings (n=10). Patients with CNL alone or CNL with HS who underwent resective surgery had good seizure outcomes, with 4 of 5 and 9 of 11 patients respectively becoming seizure-free. The study suggests CNLs can cause drug-resistant epilepsy and resective surgery may be an effective treatment for select patients































































































