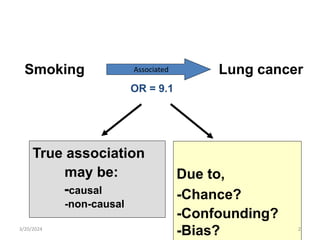
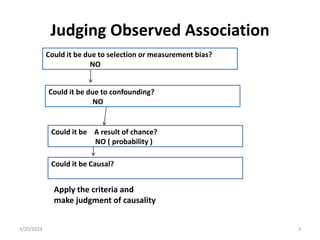
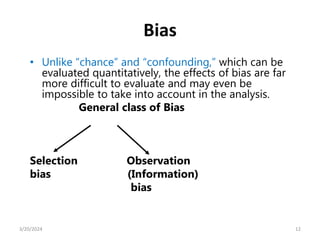
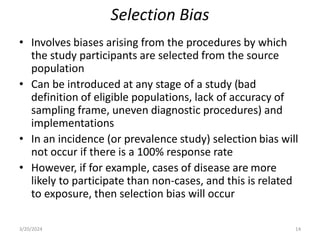
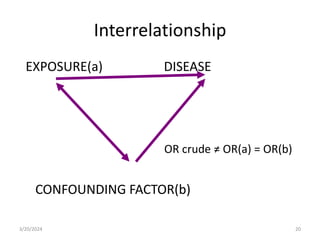
This document discusses evaluating the causality of observed associations between exposures and health outcomes. It describes several criteria for determining if an association is likely causal or non-causal, including strength of association, consistency across studies, existence of a biological gradient, temporal sequence of exposure preceding outcome, biological plausibility, coherence with other knowledge, and lack of alternative explanations such as bias or confounding. Key biases and issues that can distort observed associations are also outlined, such as selection bias, information bias, chance, and confounding variables.