Downloaded 96 times




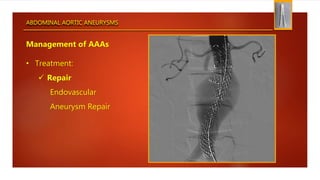
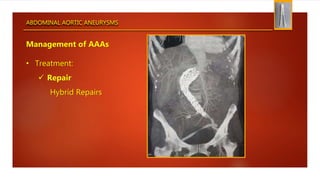



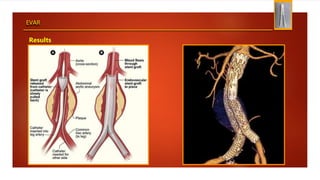

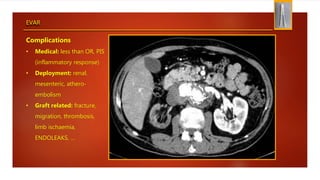
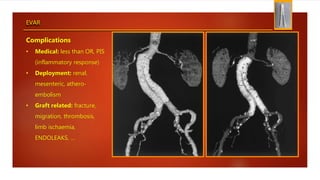
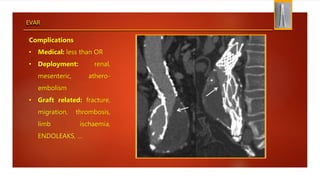
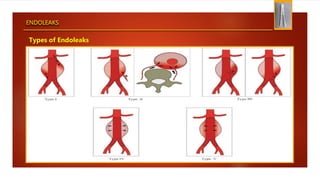

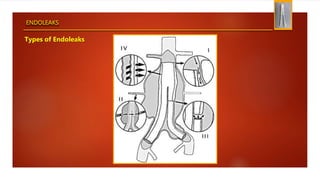
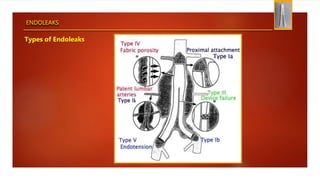
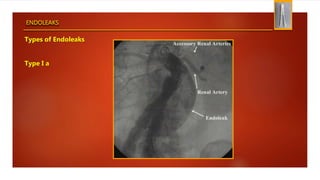


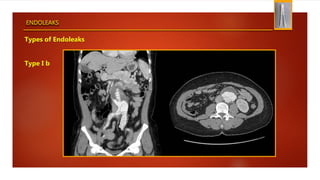

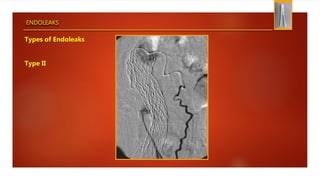
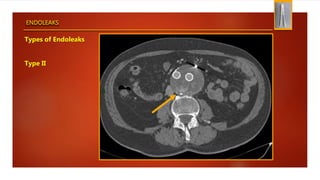
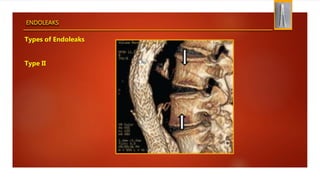
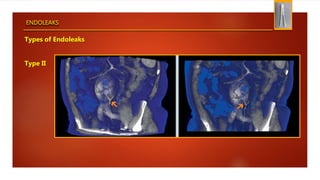
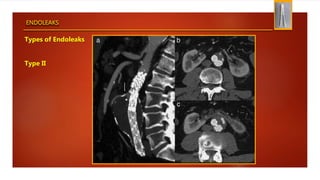
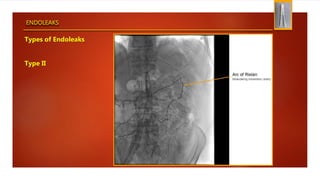

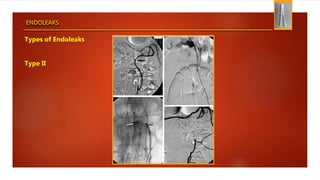
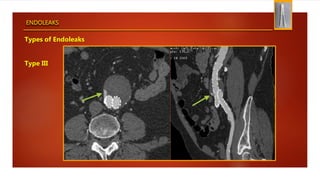
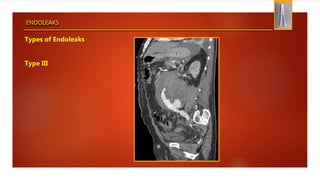
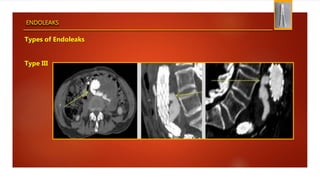
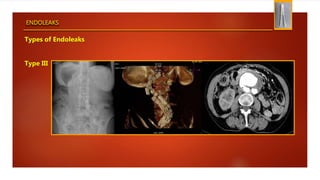



The document discusses endovascular aneurysm repair (EVAR) for abdominal aortic aneurysms. It presents a case of a 62-year-old male undergoing EVAR for a 5.5cm AAA. EVAR involves deploying a graft via catheter to exclude the aneurysm from blood flow. Complications can include endoleaks, where blood leaks outside the graft but within the aneurysm sac. The main types of endoleaks are type I (inadequate seal at graft ends), type II (collaterals inside the sac), and type III (graft component disruption). EVAR has advantages over open repair like less invasiveness but risks like increased reintervention rates.



































































