HCV
Hepatitis Cis an infection caused by the HCV that attacks the
liver and leads to inflammation. The WHO estimates that
about 3% of the world’s population has been infected with
HCV and that there are more than 170 million chronic
carriers who are at risk of developing liver cirrhosis and/or
liver cancer.
The prevalence of HCV infection varies throughout the
world. For example, Frank et al reported in 2000 that Egypt
had the highest number of reported infections, largely
attributed to the use of contaminated parenteral
antischistosomal therapy.]
This led to a mean prevalence of
anti-HCV in persons in Egypt of 22%.
4.
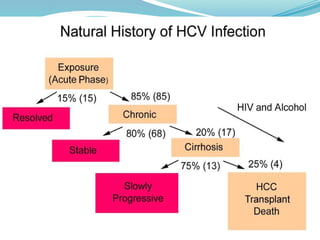
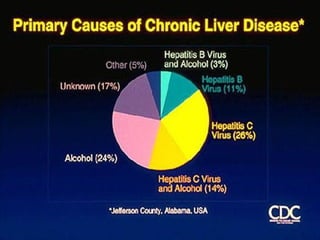
Most patientsinfected with HCV have chronic liver disease, which can progress to
cirrhosis and HCC. Chronic infection with HCV is one of the most important causes
of chronic liver disease (see the image below) and, according to a report by Davis
et al, the most common indication for orthotopic liver transplantation in the USA.
Most patients with acute and chronic infection are asymptomatic. chronic HCV
infection and chronic active hepatitis are slowly progressive diseases and result in
severe morbidity in 20-30% of infected persons.
Although acute hepatitis C virus (HCV) infection is usually mild, chronic hepatitis
results in at least 75% of patients.
Liver enzyme levels may be in the reference range, the presence of persistent
HCV-RNA levels discloses chronic infection.
Biopsy samples of the liver may reveal chronic liver disease in patients.
Cirrhosis develops in 20-50% of patients with chronic HCV infection. HCC occurs
in 11-19% of patients.
6.
Etiology
HCV, isa spherical, enveloped, single-stranded RNA virus belonging to the
Flaviviridae family and Flavivirus genus. The natural targets of HCV are
hepatocytes and, possibly, B lymphocytes. Viral clearance is associated
with the development and persistence of strong virus-specific responses
by cytotoxic T lymphocytes and helper T cells.
In most infected people, viremia persists and is accompanied by variable
degrees of hepatic inflammation and fibrosis. Findings from studies
suggest that at least 50% of hepatocytes may be infected with HCV in
patients with chronic HCV.
RNA-dependent RNA polymerase, an enzyme critical in HCV replication,
lacks proofreading capabilities and generates a large number of mutant
viruses known as quasispecies. These represent minor molecular
variations with only 1-2% nucleotide heterogeneity. HCV quasispecies pose
a major challenge to immune-mediated control of HCV and may explain
the variable clinical course and the difficulties in vaccine development.
8.
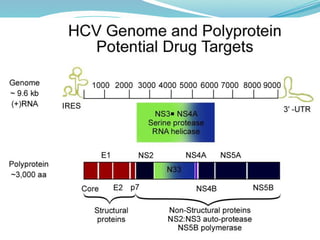
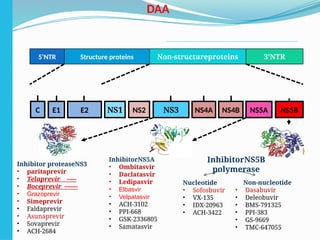
Structural componentsinclude the core and 2 envelope
proteins, E1 and E2. Two regions of the E2 protein, designated
hypervariable regions 1 and 2, have an extremely high rate of
mutation, thought to result from selective pressure by virus-
specific antibodies. The envelope protein E2 also contains the
binding site for CD-81, a tetraspanin receptor expressed on
hepatocytes and B lymphocytes that acts as a receptor or
coreceptor for HCV.
The nonstructural components include NS2, NS3, NS4A, NS4B,
NS5A, NS5B, and p7, whose proteins function as helicase-,
protease-, and RNA-dependent RNA polymerase, although the
exact function of p7 is unknown. One region within NS5A is
linked to an interferon (IFN) response and is called the IFN
sensitivity–determining region. These enzymes are critical in
viral replication and are attractive targets for future antiviral
therapy.
9.
Genotypes
HCV genomicanalysis by means of arduous gene sequencing
of many viruses has led to the division of HCV into 6 genotypes
based on homology.
Molecular differences between genotypes are relatively large,
and they have a difference of at least 30% at the nucleotide
level.
The major HCV genotype worldwide is genotype 1, which
accounts for 40-80% of all isolates. Genotype 1 also may be
associated with more severe liver disease and a higher risk of
HCC. Genotypes 1a and 1b are prevalent in the United States,
whereas in other countries, genotype 1a is less frequent.
10.
Genotypes
Genotype 1aoccurs in 50-60% of patients in the USA
Genotype 1b occurs in 15-20% of patients in the USA; this type is
most prevalent in Europe, Turkey, and Japan
Genotype 1c occurs in less than 1% of patients in the USA
Genotypes 2a, 2b, and 2c occur in 10-15% of patients in the USA;
these subtypes are widely distributed and are most responsive to
medication
Genotypes 3a and 3b occur in 4-6% of patients in the USA; these
subtypes are most prevalent in India, Pakistan, Thailand,
Australia, and Scotland
Genotype 4 occurs in less than 5% of patients in the USA; it is most
prevalent in the Middle East and Africa
Genotype 5 occurs in less than 5% of patients in the USA; it is most
prevalent in South Africa
Genotype 6 occurs in less than 5% of patients in the USA; it is most
prevalent in Southeast Asia, particularly Hong Kong and Macao
11.
Epidemiology
Transfusion ofblood contaminated with HCV was once
an important source of transmission. With the use of
PCR, Stramer et al reported that the risk of acquiring
HCV from blood transfusions is estimated to be 1 in
230,000 donations. The newer assays have decreased
the window after infection to 1-2 weeks.
Persons who inject illegal drugs with nonsterile
needles or who snort cocaine with shared straws are at
highest risk for HCV infection. In developed countries,
most new HCV infections are related to intravenous
drug abuse (IVDA).
12.
Epidemiology
Transmission ofHCV to health care workers may occur via needle-stick injuries
or other occupational exposures. Needle-stick injuries in the health care setting
result in a 3% risk of HCV transmission.
Nosocomial patient-to-patient transmission may occur by means of a
contaminated colonoscope, via dialysis, or during surgery, including organ
transplantation before 1992.
HCV may also be transmitted via tattooing, sharing razors, and acupuncture.
The uncommon routes of transmission, which affect less than 5% of the
individuals at risk, include high-risk sexual activity and maternal-fetal
transmission.
Coinfection with HIV type 1 appears to increase the risk of both sexual and
maternal-fetal transmission of HCV.
Casual household contact and contact with the saliva of those infected are
inefficient modes of transmission.
13.
Epidemiology
Worldwide, morethan 170 million persons have HCV infection. The
prevalence rates in healthy blood donors are 0.01-0.02% in the United
Kingdom and northern Europe, 1-1.5% in southern Europe, and 6.5% in
parts of equatorial Africa. Prevalence rates as high as 22% are reported
in Egypt and are attributed to the use of parenteral antischistosomal
therapy.
In the USA, HCV infection is more common among minority populations,
such as black and Hispanic persons, than other populations, in
association with lower economic status and educational levels.
In the third National Health and Nutrition Examination Survey, neither
sex nor racial-ethnic group was independently associated with HCV
infection.
Those who acquire the infection at a younger age have a somewhat
better prognosis than those who are infected later in life. Infection is
uncommon in persons aged 20 years and younger and is more prevalent
in persons older than 40 years
14.
Prognosis
Infection withHCV is self-limited in only a small minority of infected
persons. Chronic infection develops in 70-80% of patients
Cirrhosis develops within 20 years of disease onset in 20% of persons
with chronic infection.
The onset of chronic HCV infection early in life often leads to less
serious consequences.[
HBV coinfection, iron overload, and alpha 1-antitrypsin deficiency
may promote the progression of chronic HCV infection to HCV-related
cirrhosis.
The risk of cirrhosis and HCC doubles in patients who acquired HCV
infection via transfusion.
The rate and likelihood of progression is influenced by alcohol use,
immunosuppression, sex, iron status, concomitant hepatitis, and age
of acquisition
15.
Patient whoachieved an undetectable HCV viral load
had a decreased risk of subsequent liver morbidity
and death. Viral load suppression reduced the risk for
future liver events by 27%, as well as reduced the
risk of death by 45%, relative to patients who did not
achieve viral load suppression.
The risk for all liver events and death was higher in
white patients relative to black patients, and
those with HCV genotype 3 had a higher risk for all
study outcomes compared with patients who had
HCV genotype 2 (lowest risk) or 1
16.
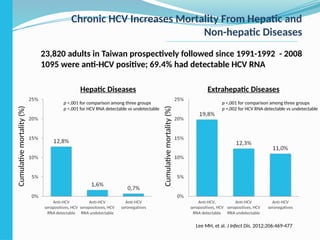
Chronic HCV IncreasesMortality From Hepatic and
Non-hepatic Diseases
23,820 adults in Taiwan prospectively followed since 1991-1992 - 2008
1095 were anti-HCV positive; 69.4% had detectable HCV RNA
Hepatic Diseases Extrahepatic Diseases
Cumulative
mortality
(%)
p <,001 for comparison among three groups
p <,001 for HCV RNA detectable vs undetectable
p <,001 for comparison among three groups
p =,002 for HCV RNA detectable vs undetectable
Lee MH, et al. J Infect Dis. 2012;206:469-477
Cumulative
mortality
(%)
17.
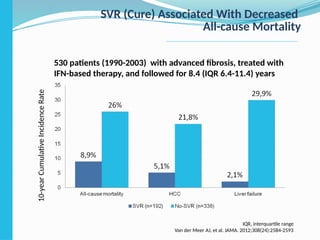
SVR (Cure) AssociatedWith Decreased
All-cause Mortality
530 patients (1990-2003) with advanced fibrosis, treated with
IFN-based therapy, and followed for 8.4 (IQR 6.4-11.4) years
10-year
Сumulative
Incidence
Rate
IQR, interquartile range
Van der Meer AJ, et al. JAMA. 2012;308(24):2584-2593
18.
Symptoms
Most patientswith chronic HCV infection are asymptomatic or may
have nonspecific symptoms such as fatigue or malaise in the
absence of hepatic synthetic dysfunction.
Patients with decompensated cirrhosis frequently have symptoms
typically observed in other patients with decompensated liver
disease, such as sleep inversion and pruritus.
Symptoms characteristic of complications from advanced or
decompensated liver disease are related to synthetic dysfunction
and portal hypertension. These include mental status changes
(hepatic encephalopathy), ankle edema and abdominal distention
(ascites), and hematemesis or melena (variceal bleeding).
Symptoms often first develop as clinical findings of extrahepatic
manifestations of HCV and most commonly involve the joints,
muscle, and skin. 74% of medical workers with HCV infection
demonstrated extrahepatic manifestations
19.
Symptoms
Arthralgias (23%)
Paresthesias (17%)
Myalgias (15%)
Pruritus (15%)
Sicca syndrome (11%)
Sensory neuropathy (9%)
Risk factors for manifestations of extrahepatic chronic HCV
infection include advanced age, female sex, and liver fibrosis.
Patients also present with symptoms that are less specific.
(pruritus and urticaria).
Patients with an organ failure can present with symptoms and
signs in the skin. Pruritus, dryness, palmar erythema, and
yellowing of the eyes and skin are examples of less specific findings
in patients with end-stage liver disease with cirrhosis
20.
Symptoms
Most patientswith HCV infection do not have abnormal physical
examination findings until they develop portal hypertension or
decompensated liver disease. One exception is patients with
extrahepatic manifestations of HCV infection, such as porphyria
cutanea tarda or necrotizing vasculitis.
Signs in patients with decompensated liver disease:
Hand signs - Palmar erythema, Dupuytren contracture, asterixis,
leukonychia, clubbing
Head signs - Icteric sclera, temporal muscle wasting, enlarged parotid,
cyanosis
Fetor hepaticus
Gynecomastia, small testes
Abdominal signs - Paraumbilical hernia - ascites, caput medusae,
hepatosplenomegaly, abdominal bruit
Ankle edema
Scant body hair
Skin signs - Spider nevi, petechiae, excoriations due to pruritus
21.
Extrahepatic manifestations
Cryoglobulinemia:
Membranoproliferative glomerulonephritis
Idiopathic thrombocytopenic purpura
Lichen planus
Keratoconjunctivitis sicca
Raynaud syndrome
Sjogren syndrome
Porphyria cutanea tarda
Necrotizing cutaneous vasculitis
Non-Hodgkin lymphoma
Approximately 10-15% of affected patients have symptoms such
as weakness, arthralgias, and purpura; these are often related to
vasculitis. The precise pathogenesis of these extrahepatic
complications has not been determined, although most are the
22.
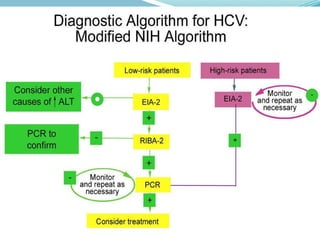
Laboratory diagnostic
Serologicscreening for HCV involves an enzyme immunoassay
(Anti-HCV, EIA). These assays are 97% specific but cannot
distinguish acute from chronic infection. s
The recombinant immunoblot assay is used to confirm HCV
infection.
Health care personnel who sustain a needle-stick injury
involving an HCV-infected patient should undergo PCR testing
for HCV immediately and then every 2 months for 6 months.
Genotyping is helpful for predicting the likelihood of response
and duration of treatment.
Genotyping can be performed by direct sequence analysis,
reverse hybridization to genotype-specific oligonucleotide
probes, or restriction fragment length polymorphisms (RFLPs).
24.
Laboratory diagnostic
CBCwith differential (10% thrombocytopenia)
Liver function tests, including ALT level
Thyroid function studies (Low thyroxine levels - in approximately 10% ),
HCV Genotyping is helpful for predicting the likelihood of response
and duration of treatment. Genotyping can be performed by direct
sequence analysis, reverse hybridization to genotype-specific
oligonucleotide probes, or restriction fragment length polymorphisms
(RFLPs).
Quantitative HCV RNA assay
Screening tests for co-infection with HIV or HBV)
Screening for alcohol abuse, drug abuse, and/or depression
The single-nucleotide polymorphism (SNP) rs12979860, located near
the IL28B gene on chromosome 19, which encodes type III interferon,
is associated with more than a 2-fold difference in the rate of sustained
virologic response to antiviral treatment with peg-IFN and ribavirin.
This SNP can be detected by PCR and is an independent predictor of
SVR response regardless of HCV genotype
25.
Laboratory diagnostic
Cryoglobulinsare found in as many as 50% of persons
with HCV infection. Vasculitis, arterial hypertension,
purpura, lichen planus, arthralgias, and low thyroxine
levels were associated with titers positive for
cryoglobulin.
Serologic findings in patients with chronic HCV infection
:
Antinuclear antibody (ANA; 41%)
Rheumatoid factor (38%)
Anticardiolipin antibody (27%)
Antithyroid antibody (13%)
Anti–smooth muscle antibody (9%)
26.
Liver biopsy
Liverbiopsy is not considered mandatory before
the initiation of treatment, but it may be helpful for
assessing the activity and severity of HCV-related
liver disease. However, some experts recommend
biopsy only in the following situations:
The diagnosis is uncertain
Other co-infections or disease may be present
The patient being considered for treatment has
normal liver enzyme levels and no extrahepatic
manifestations
The patient is immunocompromised
27.
Liver biopsy
Lymphocyticinfiltration, moderate degrees of inflammation and necrosis,
and portal or bridging fibrosis are noted. Regenerative nodules are seen in
patients with cirrhosis. Some patients also may have findings indicative of
HCC.
Most pathologists give separate measurements of disease activity (grade)
and fibrosis (stage). Many scoring systems are used, including the Ishak (6-
point scale) and the Knodell histologic activity index (18-point score); both
are useful for assessing improvements in histologic findings in studies but
are impractical for clinical use because of interobserver disagreement.
The METAVIR score is frequently used in European trials. This score
consists of a 3-point activity scale and 4-point fibrosis score, with good
agreement among pathologists.
Noninvasive methods of assessing hepatic fibrosis are in development.
Current serum assays are directed at measuring breakdown products of
extracellular matrix constituents (eg, glycoproteins, propeptides) and
their regulatory enzymes (eg, lysyl oxidase, lysyl hydroxylase, propyl
28.
Radiologic Studies
Aliver stiffness test (FibroScan) is available as a
noninvasive method of staging liver disease in persons
with chronic HCV.
The FDA (2014) gave marketing approval for the
Hepatiq radiologic image processing system. The
software application uses quantitative analysis of
nuclear medicine liver-spleen images to determine the
severity of liver disease and to predict clinical
outcomes.
29.
Treatment
The goalof treatment of HCV-infected persons is to reduce all-cause
mortality and liver-related health adverse consequences, including
end-stage liver disease and hepatocellular carcinoma, by the
achievement of virologic cure as evidenced by a sustained virologic
response.
Rating: Class I, Level A
Treatment is recommended for all patients with chronic HCV
infection, except those with short life expectancies that cannot be
remediated by treating HCV, by transplantation, or by other directed
therapy. Patients with short life expectancies owing to liver disease
should be managed in consultation with an expert.
Rating: Class I, Level A
Evaluation for advanced fibrosis using liver biopsy, imaging, and/or
noninvasive markers is recommended for all persons with HCV
infection, to facilitate an appropriate decision regarding HCV
treatment strategy and to determine the need for initiating additional
measures for the management of cirrhosis
Rating: Class I, Level A
32.
Эффективность противовирусной терапииHCV-
инфекции (генотип 1) за последнее десятилетие
ПегИФН-альфа
+
РБВ
БОЦ или ТЕЛ
+
ПегИФН-альфа
/РБВ
СИМ или СОФ
+
ПегИФН-альфа
/РБВ
Комби-ции
препаратов с прямым
противовирусным
действием
УВО
42-46%
УВО
66–79%
УВО
80–90%
УВО
90–100%
2005–2015
•elbasvir (50 mg)/grazoprevir(100 mg) - 12 weeks (with out NS5A
RAVs§
for elbasvir)
Rating: Class I, Level A
•ledipasvir (90 mg)/sofosbuvir (400 mg) -- 12 weeks
Rating: Class I, Level A
•paritaprevir (150 mg)/ritonavir (100 mg)/ombitasvir (25 mg) + 2р/д
dasabuvir (250 mg) + ribavirin (weight) - 12 weeks.
Rating: Class I, Level A
•simeprevir (150 mg) + sofosbuvir (400 mg) - 12 weeks.
Rating: Class I, Level A
•sofosbuvir (400 mg)/velpatasvir (100 mg) - 12 weeks
Rating: Class I, Level A
•daclatasvir (60 mg*) + sofosbuvir (400 mg) for 12 weeks
Rating: Class I, Level B
Genotype 1a Treatment-Naïve
Patients Without Cirrhosis
36.
•elbasvir (50 mg)/grazoprevir(100 mg) - 12 weeks (with out NS5A
RAVs§
for elbasvir)
Rating: Class I, Level A
•ledipasvir (90 mg)/sofosbuvir (400 mg) -- 12 weeks
Rating: Class I, Level A
•sofosbuvir (400 mg)/velpatasvir (100 mg) - 12 weeks
Rating: Class I, Level A
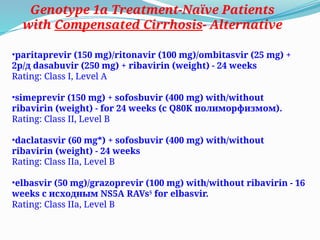
Genotype 1a Treatment-Naïve Patients with
Compensated Cirrhosis
elbasvir (50 mg)/grazoprevir (100 mg) with/without ribavirin - 16
weeks withNS5A RAVs§
for elbasvir.
Rating: Class IIa, Level B
Alternative
37.
•paritaprevir (150 mg)/ritonavir(100 mg)/ombitasvir (25 mg) +
2р/д dasabuvir (250 mg) + ribavirin (weight) - 24 weeks
Rating: Class I, Level A
•simeprevir (150 mg) + sofosbuvir (400 mg) with/without
ribavirin (weight) - for 24 weeks (с Q80K полиморфизмом).
Rating: Class II, Level B
•daclatasvir (60 mg*) + sofosbuvir (400 mg) with/without
ribavirin (weight) - 24 weeks
Rating: Class IIa, Level B
•elbasvir (50 mg)/grazoprevir (100 mg) with/without ribavirin - 16
weeks с исходным NS5A RAVs§
for elbasvir.
Rating: Class IIa, Level B
Genotype 1a Treatment-Naïve Patients
with Compensated Cirrhosis- Alternative
38.
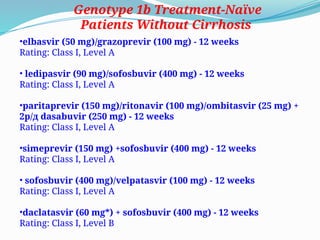
•elbasvir (50 mg)/grazoprevir(100 mg) - 12 weeks
Rating: Class I, Level A
• ledipasvir (90 mg)/sofosbuvir (400 mg) - 12 weeks
Rating: Class I, Level A
•paritaprevir (150 mg)/ritonavir (100 mg)/ombitasvir (25 mg) +
2р/д dasabuvir (250 mg) - 12 weeks
Rating: Class I, Level A
•simeprevir (150 mg) +sofosbuvir (400 mg) - 12 weeks
Rating: Class I, Level A
• sofosbuvir (400 mg)/velpatasvir (100 mg) - 12 weeks
Rating: Class I, Level A
•daclatasvir (60 mg*) + sofosbuvir (400 mg) - 12 weeks
Rating: Class I, Level B
Genotype 1b Treatment-Naïve
Patients Without Cirrhosis
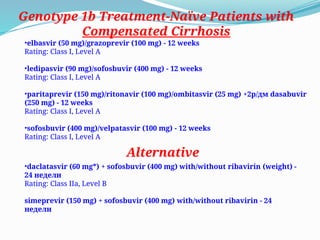
39.
•elbasvir (50 mg)/grazoprevir(100 mg) - 12 weeks
Rating: Class I, Level A
•ledipasvir (90 mg)/sofosbuvir (400 mg) - 12 weeks
Rating: Class I, Level A
•paritaprevir (150 mg)/ritonavir (100 mg)/ombitasvir (25 mg) +2р/дм dasabuvir
(250 mg) - 12 weeks
Rating: Class I, Level A
•sofosbuvir (400 mg)/velpatasvir (100 mg) - 12 weeks
Rating: Class I, Level A
Genotype 1b Treatment-Naïve Patients with
Compensated Cirrhosis
•daclatasvir (60 mg*) + sofosbuvir (400 mg) with/without ribavirin (weight) -
24 недели
Rating: Class IIa, Level B
simeprevir (150 mg) + sofosbuvir (400 mg) with/without ribavirin - 24
недели
Alternative
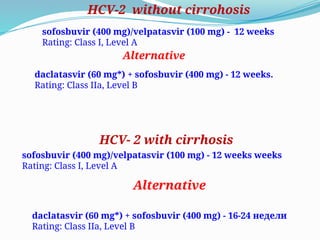
40.
sofosbuvir (400 mg)/velpatasvir(100 mg) - 12 weeks
Rating: Class I, Level A
daclatasvir (60 mg*) + sofosbuvir (400 mg) - 12 weeks.
Rating: Class IIa, Level B
HCV-2 without cirrohosis
HCV- 2 with cirrhosis
sofosbuvir (400 mg)/velpatasvir (100 mg) - 12 weeks weeks
Rating: Class I, Level A
Alternative
daclatasvir (60 mg*) + sofosbuvir (400 mg) - 16-24 недели
Rating: Class IIa, Level B
Alternative
41.
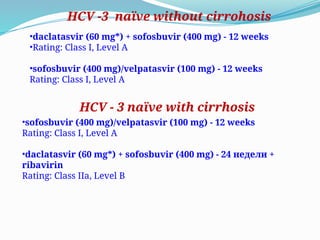
•daclatasvir (60 mg*)+ sofosbuvir (400 mg) - 12 weeks
•Rating: Class I, Level A
•sofosbuvir (400 mg)/velpatasvir (100 mg) - 12 weeks
Rating: Class I, Level A
•sofosbuvir (400 mg)/velpatasvir (100 mg) - 12 weeks
Rating: Class I, Level A
•daclatasvir (60 mg*) + sofosbuvir (400 mg) - 24 недели +
ribavirin
Rating: Class IIa, Level B
HCV -3 naïve without cirrohosis
HCV - 3 naïve with cirrhosis
42.
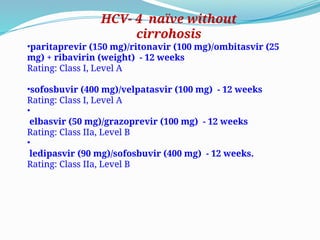
•paritaprevir (150 mg)/ritonavir(100 mg)/ombitasvir (25
mg) + ribavirin (weight) - 12 weeks
Rating: Class I, Level A
•sofosbuvir (400 mg)/velpatasvir (100 mg) - 12 weeks
Rating: Class I, Level A
•
elbasvir (50 mg)/grazoprevir (100 mg) - 12 weeks
Rating: Class IIa, Level B
•
ledipasvir (90 mg)/sofosbuvir (400 mg) - 12 weeks.
Rating: Class IIa, Level B
HCV- 4 naïve without
cirrohosis
43.
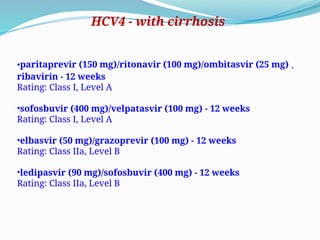
•paritaprevir (150 mg)/ritonavir(100 mg)/ombitasvir (25 mg) +
ribavirin - 12 weeks
Rating: Class I, Level A
•sofosbuvir (400 mg)/velpatasvir (100 mg) - 12 weeks
Rating: Class I, Level A
•elbasvir (50 mg)/grazoprevir (100 mg) - 12 weeks
Rating: Class IIa, Level B
•ledipasvir (90 mg)/sofosbuvir (400 mg) - 12 weeks
Rating: Class IIa, Level B
HCV4 - with cirrhosis
44.
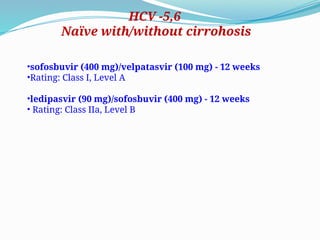
•sofosbuvir (400 mg)/velpatasvir(100 mg) - 12 weeks
•Rating: Class I, Level A
•ledipasvir (90 mg)/sofosbuvir (400 mg) - 12 weeks
• Rating: Class IIa, Level B
HCV -5,6
Naïve with/without cirrohosis
45.
If the practitionerand patient have decided that a delay in treatment
initiation is acceptable, monitoring for spontaneous clearance is
recommended for a minimum of 6 months. When the decision is made to
initiate treatment after 6 months, treating as described for chronic hepatitis
C is recommended
Rating: Class IIa, Level C
If a decision has been made to initiate treatment during the acute infection
period, monitoring HCV RNA for at least 12 weeks to 16 weeks before starting
treatment is recommended to allow for spontaneous clearance.
Rating: Class IIa, Level C
Recommended Regimens for Patients with Acute HCV Infection.
Owing to high efficacy and safety, the same regimens that are recommended
for chronic HCV infection are recommended for acute infection.
Rating: Class IIa, Level C
Acute HCV infection
Prevention
•Currently, no productsare available to prevent HCV infection. The
development of immunoprophylaxis for this disease is proving difficult;
an effective neutralizing immune response has not been demonstrated.
•Patients with hepatitis C should be advised to abstain from alcohol use;
they should also be advised to use barrier protection during sexual
intercourse. Reducing risk from shared ancillary drug preparation
equipment, such as containers, rinse water, and filters, in addition to
shared syringes
•Addressing social and relational contexts of injecting can encourage
uninfected individuals to take precautions when injecting drugs with
infected sex partners
•Developing models to guide delivery of new prevention strategies,
including already-available approaches such as increasing syringe
availability and future strategies such as direct-acting antivirals that can
be used prophylactically, as well as vaccines
Editor's Notes
#16 J Infect Dis. 2012 Aug 15;206(4):469-77. doi: 10.1093/infdis/jis385. Epub 2012 Jul 17.
Chronic hepatitis C virus infection increases mortality from hepatic and extrahepatic diseases: a community-based long-term prospective study. Lee H, Yang P, Chen C, Chen J, Huang S, Jan C, Chen T, Sun C, Wu M, Chen S, Chu K, Ho S, Lu T, Wu W, Ou T, Lin C, Shih K, Chung W, Li C, Chen C, How W.1Genomics Research Center, Academia Sinica, Taipei, Taiwan.
Abstract BACKGROUND: The study aimed to evaluate the risk of hepatitis C virus (HCV) infection on hepatic and extrahepatic deaths.
METHODS: A cohort of 23 820 adults aged 30-65 years old were enrolled during 1991-1992. The seromarkers hepatitis B surface antigen (HBsAg), anti-HCV, and serum HCV RNA levels at study entry were tested. The vital status was ascertained through computerized linkage with national death certification profiles from 1991 to 2008.
RESULTS: There were 19,636 HBsAg-seronegatives, including 18,541 anti-HCV seronegatives and 1095 anti-HCV seropositives. Among anti-HCV seropositives, 69.4% had detectable serum HCV RNA levels. There were 2394 deaths that occurred during an average follow-up period of 16.2 years. Compared with anti-HCV seronegatives, anti-HCV seropositives had higher mortality from both hepatic and extrahepatic diseases, showing multivariate-adjusted hazard ratio (95% confidence interval) of 1.89 (1.66-2.15) for all causes of death; 12.48 (9.34-16.66) for hepatic diseases; 1.35 (1.15-1.57) for extrahepatic diseases; 1.50 (1.10-2.03) for circulatory diseases; 2.77 (1.49-5.15) for nephritis, nephrotic syndrome, and nephrosis; 4.08 (1.38-12.08) for esophageal cancer; 4.19 (1.18-14.94) for prostate cancer; and 8.22 (1.36-49.66) for thyroid cancer. Anti-HCV seropositives with detectable HCV RNA levels had significantly higher mortality from hepatic and extrahepatic diseases than anti-HCV seropositives with undetectable HCV RNA.
CONCLUSIONS: Monitoring HCV RNA in anti-HCV seropositives is essential for the prediction of mortality associated with hepatitis
#17 Association Between Sustained Virological Response and All-Cause Mortality Among Patients With Chronic Hepatitis C and Advanced Hepatic Fibrosis FREE
Adriaan J. van der Meer, MD; Bart J. Veldt, MD, PhD; Jordan J. Feld, MD, PhD; Heiner Wedemeyer, MD, PhD; Jean-François Dufour, MD, PhD; Frank Lammert, MD, PhD; Andres Duarte-Rojo, MD; E. Jenny Heathcote, MD, PhD; Michael P. Manns, MD, PhD; Lorenz Kuske; Stefan Zeuzem, MD, PhD; W. Peter Hofmann, MD, PhD; Robert J. de Knegt, MD, PhD; Bettina E. Hansen, PhD; Harry L. A. Janssen, MD, PhD
JAMA. 2012;308(24):2584-2593. doi:10.1001/jama.2012.144878. ABSTRACT Objective To assess the association between sustained virological response (SVR) and all-cause mortality in patients with chronic HCV infection and advanced hepatic fibrosis.
Design, Setting, and Patients An international, multicenter, long-term follow-up study from 5 large tertiary care hospitals in Europe and Canada of 530 patients with chronic HCV infection who started an interferon-based treatment regimen between 1990 and 2003, following histological proof of advanced hepatic fibrosis or cirrhosis (Ishak score 4-6). Complete follow-up ranged between January 2010 and October 2011.Main Outcome Measures All-cause mortality. Secondary outcomes were liver failure, HCC, and liver-related mortality or liver transplantation.
Results The 530 study patients were followed up for a median (interquartile range [IQR]) of 8.4 (6.4-11.4) years. The baseline median (IQR) age was 48 (42-56) years and 369 patients (70%) were men. The Ishak fibrosis score was 4 in 143 patients (27%), 5 in 101 patients (19%), and 6 in 286 patients (54%). There were 192 patients (36%) who achieved SVR; 13 patients with SVR and 100 without SVR died (10-year cumulative all-cause mortality rate, 8.9% [95% CI, 3.3%-14.5%] with SVR and 26.0% [95% CI, 20.2%-28.4%] without SVR; P < .001). In time-dependent multivariate Cox regression analysis, SVR was associated with reduced risk of all-cause mortality (hazard ratio [HR], 0.26; 95% CI, 0.14-0.49; P < .001) and reduced risk of liver-related mortality or transplantation (HR, 0.06; 95% CI, 0.02-0.19; P < .001), the latter occurring in 3 patients with SVR and 103 without SVR. The 10-year cumulative incidence rate of liver-related mortality or transplantation was 1.9% (95% CI, 0.0%-4.1%) with SVR and 27.4% (95% CI, 22.0%-32.8%) without SVR (P < .001). There were 7 patients with SVR and 76 without SVR who developed HCC (10-year cumulative incidence rate, 5.1%; 95% CI, 1.3%-8.9%; vs 21.8%; 95% CI, 16.6%-27.0%; P < .001), and 4 patients with SVR and 111 without SVR experienced liver failure (10-year cumulative incidence rate, 2.1%; 95% CI, 0.0%-4.5%; vs 29.9%; 95% CI, 24.3%-35.5%; P < .001).
Conclusion Among patients with chronic HCV infection and advanced hepatic fibrosis, sustained virological response to interferon-based treatment was associated with lower all-cause mortality.
![HCV
Hepatitis C is an infection caused by the HCV that attacks the
liver and leads to inflammation. The WHO estimates that
about 3% of the world’s population has been infected with
HCV and that there are more than 170 million chronic
carriers who are at risk of developing liver cirrhosis and/or
liver cancer.
The prevalence of HCV infection varies throughout the
world. For example, Frank et al reported in 2000 that Egypt
had the highest number of reported infections, largely
attributed to the use of contaminated parenteral
antischistosomal therapy.]
This led to a mean prevalence of
anti-HCV in persons in Egypt of 22%.](https://image.slidesharecdn.com/hepatitisc-250424113959-c6389595/85/Hepatitis-c-presentation-for-medical-students-3-320.jpg)