HEPATITIS C INFECTION-ITRODUCTION
HepatitisC is an infection caused by the hepatitis C virus
(HCV) that attacks the liver and leads to inflammation.
About 50 million people globally have chronic hepatitis
C, with approximately 242,000 dying from this infection,
primarily due to cirrhosis and hepatocellular carcinoma
In Ghana the prevalence of HCV is estimated to be
3.3%. Prevalence is disproportionately higher in the
people of northern Ghana (8.4-14.4%)
Males are about 1.5 times more likely to be infected
than females
3.
VIRAL PROPERTIES
HCV isa positive single stranded RNA virus, classified as
family Flaviviridae, genus Hepacivirus. Various viruses
can be differentiated by RNA sequence analysis into at
least six major genotypes
The genome is 9.4 kb in size and encodes a core
protein, two envelope glycoproteins, and several
nonstructural proteins
Most new infections with HCV are subclinical. The
majority (70–90%) of HCV patients develops chronic
hepatitis, and many are at risk of progressing to chronic
active hepatitis and cirrhosis (10–20%).
4.
MODE OF TRANSMISSION
HepatitisC is primarily transmitted through exposure to
infected blood:
Injection Drug Use: Sharing needles, syringes, or other
equipment to inject drugs is the most common mode of
transmission in many countries.
Blood Transfusions and Organ Transplants: Before
widespread screening of the blood supply began in the
early 1990s, blood transfusions and organ transplants were
a significant route of transmission. Today, this mode is rare
in countries with rigorous blood screening protocols.
5.
MODE OF TRANSMISSION
Healthcare-RelatedExposures: Unsafe medical practices,
such as using non-sterile equipment, can lead to
transmission. This is more common in areas with limited
resources or inadequate healthcare practices.
Needlestick Injuries: Healthcare workers can be at risk if
they are accidentally stuck with needles that have been
used on HCV-infected patients.
Mother-to-Child Transmission: A mother infected with
HCV can transmit the virus to her baby during childbirth.
This is less common than with hepatitis B or HIV.
6.
MODE OF TRANSMISSION
SexualTransmission: While the risk of sexual transmission is
generally low, it can be higher among people with
multiple sexual partners, men who have sex with men
(especially those who are HIV-positive), and those with
sexually transmitted infections.
Tattooing and Body Piercing: If proper sterilization
techniques are not followed, needles or equipment
contaminated with infected blood can transmit HCV.
Sharing Personal Items: Items such as razors, toothbrushes,
or any other personal items that may have come into
contact with infected blood can also be a mode of
7.
PATHOLOGY OF HCV
AcuteInfection:
Initial Infection: Upon entry into the bloodstream, HCV
targets liver cells (hepatocytes) using specific receptors
to enter and replicate.
Immune Response: The immune system mounts a
response, with both innate (e.g., interferons) and
adaptive (e.g., T-cells) mechanisms attempting to clear
the virus. In about 15-25% of cases, the infection is
cleared within six months.
8.
PATHOLOGY OF HCV
ChronicInfection:
Persistence: In the remaining 75-85% of cases, HCV
evades the immune response and establishes a
chronic infection. The virus persists in the liver, causing
ongoing inflammation.
Liver Damage: Chronic inflammation leads to liver cell
injury and death (apoptosis and necrosis), resulting in
fibrosis (scarring) as the liver attempts to repair itself.
Over time, extensive fibrosis can lead to cirrhosis.
9.
PATHOLOGY OF HCV
Complications:
Cirrhosis:The end-stage of chronic liver damage,
characterized by extensive fibrosis, regenerative nodules,
and impaired liver function. Cirrhosis significantly increases
the risk of HCC.
Hepatocellular Carcinoma (HCC): Chronic HCV
infection is a major risk factor for HCC due to ongoing
liver cell turnover, DNA damage, and the pro-
inflammatory environment.
10.
PATHOGENESIS OF HCV
1.Viral Entry and Replication:
• Entry: HCV enters hepatocytes through specific receptors,
including CD81, SR-B1, claudin-1, and occludin.
• Replication: Once inside the cell, HCV uses the host's
cellular machinery to replicate. The viral RNA is translated
into a single polyprotein, which is then cleaved into
functional viral proteins.
11.
PATHOGENESIS OF HCV
2.Immune Evasion:
• Viral Mutations: HCV has a high mutation rate, which
allows it to rapidly evolve and evade immune detection.
• Interference with Immune Response: HCV proteins can
interfere with both the innate and adaptive immune
responses. For example, the NS3/4A protease can inhibit
interferon signaling pathways.
12.
PATHOGENESIS OF HCV
3.Immune-Mediated Liver Damage:
Inflammation: The immune system's response to HCV,
including cytotoxic T cells and inflammatory cytokines,
contributes to liver damage.
Fibrosis: Chronic inflammation activates hepatic stellate
cells, which produce extracellular matrix components,
leading to fibrosis.
13.
PATHOGENESIS OF HCV
OxidativeStress and Apoptosis:
Oxidative Stress: HCV infection increases oxidative stress
within hepatocytes, contributing to cell damage and
apoptosis.
Apoptosis: Programmed cell death is a common
response to HCV infection, further contributing to liver
injury and inflammation.
14.
CLINICAL DISEASE
Hepatitis CVirus (HCV) infection can present with a range of
signs and symptoms, varying between acute and chronic stages.
1. Acute HCV Infection
Acute HCV infection often goes unnoticed because it is usually
asymptomatic or presents with mild, non-specific symptoms.
When symptoms do occur, they may include:
• Fatigue: General feeling of tiredness and lack of energy.
• Fever: Mild to moderate increase in body temperature.
• Nausea and Vomiting: Feeling sick to the stomach and vomiting.
15.
CLINICAL DISEASE
• Lossof Appetite: Reduced desire to eat.
• Abdominal Pain: Pain or discomfort, particularly in the
upper right quadrant of the abdomen where the liver is
located.
• Dark Urine: Urine that is darker than usual.
• Jaundice: Yellowing of the skin and eyes due to
elevated bilirubin levels.
• Joint Pain: Aches and pains in the joints.
16.
CLINICAL DISEASE
Advanced LiverDisease
In cases where chronic HCV infection has led to significant liver
damage, such as cirrhosis or liver failure, more severe symptoms
and complications may occur:
• Ascites: Accumulation of fluid in the abdomen, leading to swelling.
• Edema: Swelling in the legs, ankles, and feet due to fluid retention.
• Bruising and Bleeding: Increased tendency to bruise or bleed easily,
due to impaired liver function.
• Encephalopathy: Confusion, memory problems, and difficulty
concentrating due to the buildup of toxins in the blood affecting
the brain.
17.
CLINICAL DISEASE
Spider Angiomas:Small, spider-like blood vessels visible under the
skin.
Palmar Erythema: Reddening of the palms.
Gynecomastia: Enlargement of breast tissue in men.
Portal Hypertension: Increased blood pressure in the portal vein
leading to varices (enlarged veins) in the esophagus and
stomach, which can bleed.
Asymptomatic Cases
A significant number of individuals with HCV remain asymptomatic,
especially during the early stages of infection. This lack of symptoms
contributes to the high rates of undiagnosed and untreated HCV
infections, emphasizing the importance of screening and early
detection, particularly in high-risk populations.
18.
DIAGNOSIS
• HCV AntibodyTest (Anti-HCV): (Initial Screening)
• Purpose: Detects antibodies produced by the immune system in response to
HCV infection.
• Interpretation:
• Positive: Indicates past or present infection.
• Negative: No evidence of past or present infection.
Other Tests
HCV RNA Test (PCR Test)-Confirmatory
HCV Genotyping - Important in tailoring antiviral
Liver Function Tests (LFTs)- Establishing liver injury by virus
Abdominal Ultrasound scan: Non-invasive diagnosis of liver fibrosis or
cancer
Liver Biopsy: Establishes fibrosis and or liver cancer
19.
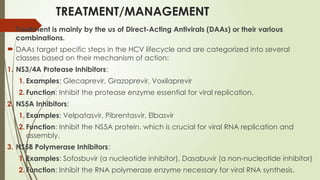
TREATMENT/MANAGEMENT
Treatment ismainly by the us of Direct-Acting Antivirals (DAAs) or their various
combinations.
DAAs target specific steps in the HCV lifecycle and are categorized into several
classes based on their mechanism of action:
1. NS3/4A Protease Inhibitors:
1. Examples: Glecaprevir, Grazoprevir, Voxilaprevir
2. Function: Inhibit the protease enzyme essential for viral replication.
2. NS5A Inhibitors:
1. Examples: Velpatasvir, Pibrentasvir, Elbasvir
2. Function: Inhibit the NS5A protein, which is crucial for viral RNA replication and
assembly.
3. NS5B Polymerase Inhibitors:
1. Examples: Sofosbuvir (a nucleotide inhibitor), Dasabuvir (a non-nucleotide inhibitor)
2. Function: Inhibit the RNA polymerase enzyme necessary for viral RNA synthesis.

























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







