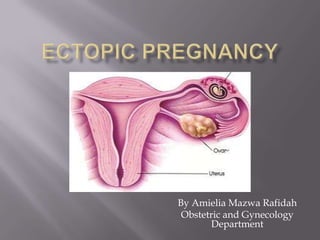
2. An ectopic pregnancy is a gestation that
implants outside of the endometrial cavity.
@
defined as pregnancy occurring outside the
endometrial lining of the uterus
It represents a serious hazard to a woman’s
health and reproductive potential, requiring
prompt recognition and early aggressive
intervention.
3. 95% occur in the tubes: the commonest site is the Ampulla
(85%), followed by the Isthmus.
The uterus:
I. Intramural.
II. Angular
III. Cervical
IV. Rudimentary Horn
The Ovary
Broad Ligament
Abdominal:
I. Primary: first implantation occurs in a peritoneal surface.
II. Secondary: original implantation occurs first in the tube-ostia,
aborted subsequently then reimplanted into a peritoneal surface.
Multiple Ectopic: may occur:
Involving both tubes
Combined intra- & extra-uterine pregnancy
4.
5.
6.
7. Since the early 1970s, the incidence of ectopic
pregnancy has tripled, and currently this
condition represents the fourth leading cause
of maternal mortality overall (4%) and the most
common cause of maternal mortality in the first
trimester.
The overall incidence of ectopic pregnancy is
estimated to be at least one in every 200
pregnancies.
8. Probably as many as 50% of cases result from
alteration of tubal transport mechanisms
secondary to damage to the ciliated surface of
the endosalpinx caused by infections such as
Chlamydia and gonorrhea.
Others are the result of intrinsic abnormalities
of the fertilized ovum and possibly
transmigration of the oocyte to the contralateral
tube, with resulting delays in passage.
9. Tubal pregnancies rapidly invade the mucosa,
feeding from the tubal vessels, which become
enlarged and engorged.
The segment of the affected tube is distended
as the pregnancy grows.
Possible outcomes of such abnormal gestations
are as follows:
10. The pregnancy is unable to survive owing to its
poor blood supply, thus resulting in a tubal
abortion and resorption , or it is expelled from
the fimbriated end into the abdominal cavity.
The pregnancy continues to grow until the
overdistended tube ruptures, which resulting
profuse intraperitoneal bleeding.
11. In rare instances, a tubal pregnancy will be
expelled from the tube and seed onto sites in
the abdominal cavity (e.g. the omentum, the
small/large bowel, or the parietal peritoneum),
and gives rise to a viable abdominal pregnancy
12. High risk factors can be summarized as follows:
A history of tubal infection (ectopic rate of 1:24,
as opposed to 1:200 in non infected patients)
Prior ectopic pregnancy (15% to 50% increase
in incidence of ectopic gestation in subsequent
pregnancies)
History of tubal sterilization within the past 1
to 2 years (higher incidence if cauterization was
used)
13. History of tubal reconstructive surgery
(tuboplasty or end-to-end reanastomosis for
sterilization reversal)
Pregnancy with an IUD in place or a history of
IUD use.
Infertility.
More than one therapeutic abortion
(controversial)
Pregnancy resulting from failed postcoital
contraception (probably associated with
abnormal tubal transport)
14.
15. The classic symptom triad
amenorrhea,
vaginal
bleeding,
abdominal pain
normal pregnancy findings like breast
tenderness, nausea and urinary frequency are
also found.
16. Abdominal pain, usually in the lower abdomen
in early cases, or generalized in ruptured
ectopics with a hemoperitoneum.
Amenorrhea or a history of an abnormal last
menstrual period is found in 75% to 90% of
ectopic pregnancies.
Vaginal bleeding, from spotting to the
equivalent of a menstrual period, results from a
low human chorionic gonadotropin (hCG)
production by the ectopic trophoblast and is
seen in 50% to 80% of patients.
17. Making the diagnosis of an acutely ruptured
ectopic pregnancy is fairly straightforward.
The patient presents with symptoms of
increasing abdominal pain, abdominal
distention, and hypovolemia.
The entire abdomen is acutely tender with
guarding and rebound tenderness
18. in patients with an unruptured ectopic pregnancy
may be extremely variable.
90% have abdominal tenderness, but
only 45% have positive rebound tenderness, and
only 50 % have an adnexal mass on pelvic examination.
In half the cases, the mass is contralateral to the
ectopic pregnancy and represents the corpus
luteum.
20%present with bilateral adnexal masses owing to
the presence of a contralateral coupus luteum cyst.
The uterus is soft and either of normal size or
slightly enlarged.
19. Many gynecologic and nongynecologic
disorders have symptoms in common with
ectopic pregnancy.
Gynecologic disorders to be considered include :
Threatened or incomplete abortion
A ruptured corpus luteum cyst
Acute pelvic inflammatory disease with fever,
abdominal pain, leukocytosis, and, at times, adnexal
masses.
Adnexal torsion
Degenerating leiomyoma (common in pregnancy)
20. The key to the successful management of
ectopic pregnancy is early diagnosis.
Although the number of new cases has
increased threefold, fewer are arriving at the
hospital ruptured, with the patient already in
hemorrhagic shock.
This decrease is evidence that a high index of
suspicion and vigorous efforts at early
diagnosis are effective.
21. Human chorionic gonadotropin is consisting of
two linked subunits, α and β
β-hCG is secreted by both the cytotrophoblast
and the syncytiotrophoblast and has the sole
function of supporting the corpus luteum.
Abnormal β-hCG could not provide
information on the location of the pregnancy.
Ultrasonography must be used to locate the
gestation.
22. its application to the diagnosis of ectopic
pregnancy, alone and in combination with hCG
testing, is now the standard of care.
Transvaginal ultrasonography has allowed the
detection of an intrauterine gestational sac at as
early as 5 weeks of amenorrhea (2 mm
diameter).
23. If the sac is not visualized at the uterine cavity,
special attention is needed to differentiate
between a true sac and a pseudosac, which is a
ring-like structure produced on ultrasound by
a prominent decidual echo.
Evidence of hemoperitoneum may be inferred
by the sonographic description of “free fluid in
the cul-de-sac.”
24.
25. Culdocentesis is the technique by which a
needle, attached to a syringe, is inserted
transvaginally through the posterior vaginal
fornix into the pouch of Douglas to detect any
fluid within the peritoneal cavity
Although the procedure is simple, inexpensive,
and rapid, it is quite uncomfortable for the
patient and is of limited use in an unruptured
ectopic pregnancy.
It is unnecessary when the diagnosis is obvious
and has a high false-negative rate.
29. Immediate surgery is indicated when the
diagnosis of ectopic pregnancy with
hemorrhage is made.
Transfusion with whole blood or an
appropriate blood component therapy as soon
possible is indicated when the patient is in
shock.
30. Rapid entry into the abdomen should be
accomplished, as control of hemorrhage can be
lifesaving.
Careful, fast exploration of the abdominal
cavity should be done at once.
Remove products of conception, clots, and free
blood.
At operation the damaged tube is usually
removed.
This procedure is the most common for ectopic
pregnancy.
31. The type of procedure performed by either
laparoscopy or laparotomy will be dictated by
local findings at the time of surgery and the
desire of the woman for future fertility.
In patients who with to conserve fertility, a
linear salpingostomy is the treatment of choice
in unruptured ampullary pregnancies.
In ampullary pregnancies that have already
ruptured, a segmantal resection or partial
salpingectomy can be offered, which implies
the removal of only the affected segment of
tube, leaving the rest intact.
32.
33.
34.
35. Unruptured ectopic pregnancy can be treated
with Methotrexate (MTX).
36. no contraidications to MTX
type of unruptured or abortion
unruptued mass <4 cm at its greastest
dimension
β-hCG level <2000mIU/ml
without signs of hemoperitoneum
37.
38. ABSOLUTE
Breast feeding.
Immunodeficiency
Alcoholism or related Hepatic Cirrhosis.
MTX sensitivity.
Active pulmonary disease.
Peptic Ulcer disease.
Hepatic, Renal or Hematologic dysfunction.
RELATIVE
Gestational Age >3.5 cm,
Embryonic HR present.
39. As many as 80% of ectopic pregnancies with
hCG levels of 1000mIU/ml or less will not
rupture spontaneously or bleed profusely but
will undergo spontaneous resolution.
Expectant management is generally reserved
for reliable, relatively asymptomatic patients in
whom the hCG titers are <200mIU/ml and
delining.
40. Ectopic pregnancy and tubal pregnancy are
terms used interchangeably because other sites
of ectopic implantation are rare.
A pregnancy can implant on the surface of the
ovary.
The treatment is aimed at removing the
pregnancy and sacrificing as little as possible of
the ovarian tissue.
41. Cervical pregnancy usually presents with
profuse vaginal bleeding, and attempts at
removal of the pregnancy are often
unsuccessful.
Hysterectomy is frequently indicated and is
usually quite difficult.
In more recent years, methotrexate have been
used to manage cervical pregnancy.
42. http://en.wikipedia.org/wiki/Ectopic_pregnancy
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001897/
http://www.google.com/imgres?q=ectopic+pregnancy
American College of Obstetricians and Gynecologists.
Management of recurrent and early pregnancy loss. ACOG
Practice Bulletin No. 24. Obstet Gynecol . 2001; 97 (2).
American College of Obstetricians and Gynecologists. Medical
management of abortion.
ACOG Practice Bulletin No. 67. Obstet Gynecol . 2005;106
(4):871-882.
American College of Obstetricians and Gynecologists. Medical
Management of tubal pregnancy.
ACOG Practice Bulletin No. 3. Obstet Gynecol . 1998;92(6):1-7.