Downloaded 10 times


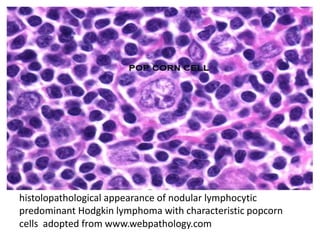

A 12-year-old female patient was diagnosed with Hodgkin lymphoma, nodular lymphocytic predominant type, after initially presenting with abdominal pain and cervical lymphadenopathy. She underwent treatment consisting of 4 courses of ABVD/COEP and radiation, achieving complete response, and has been in remission for over 2.5 years with ongoing follow-up. The document raises questions regarding treatment decisions and the role of PET-CT in managing her condition.

















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

















