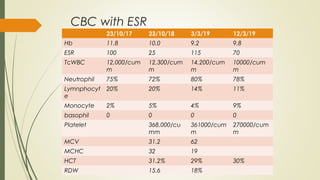
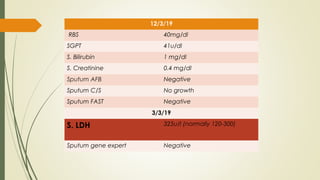
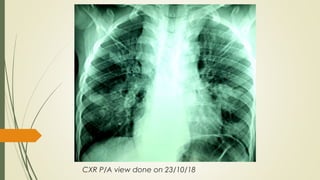
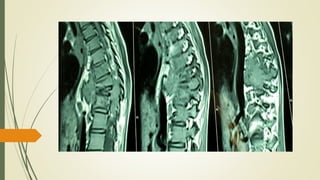
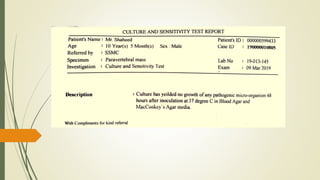
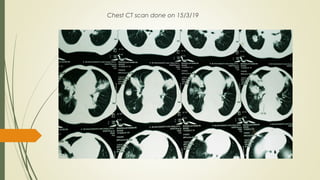
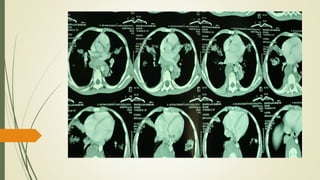
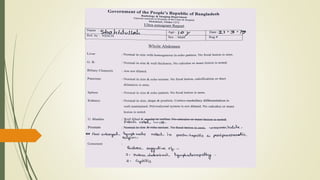
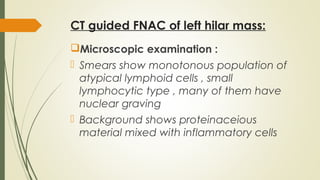
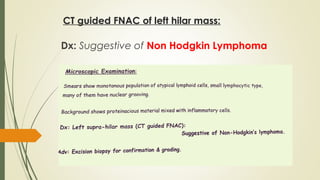
This document describes the case of a 10-year-old boy who presented with back pain and swelling for 1.5 years. Initial x-rays led to a diagnosis of spinal tuberculosis, but anti-tuberculosis treatment did not improve his condition. He then developed a cough. Further investigations including CT scans and biopsies revealed non-Hodgkin lymphoma with lymph node and lung involvement. Non-Hodgkin lymphoma can mimic other conditions at presentation and this case illustrates the importance of thorough investigation and follow-up given lack of response to initial treatment.




















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




