The document provides information about the peritoneum:
1. The peritoneum is a serous membrane that lines the abdominal cavity and is divided into a parietal layer covering the abdominal wall and a visceral layer adhered to organs.
2. It is composed of an outer fibrous layer and inner mesothelial cells that secrete fluid for lubrication.
3. Folds of peritoneum suspend organs in the abdomen and provide pathways for vessels, nerves and lymphatics.
gallbladder and the structure associated, hepatic duct, cystic duct, bile dduct, common bile duct, ampula of vater, sphincter of oddi, parts of gall bladder, relation of gall bladder, relation of Common bile duct, complication of bile stone, parts of CBD, blood supply of gall bladder, innervation of gall bladder, blood supply of common bile duct,lymphatic drainage of bile duct and gall bladder
anatomy of duodenum, location or position of duodenum, parts of duodenum, relations of each parts of duodenum, ligaments of treitz, visceral and peritoneal relation of duodenum, blood supply of duodenum, innervation of duodenum, clinical aspects of duodenum, duodenal ulcer, diverticulum, deodinitis, duodenal obstruction
gallbladder and the structure associated, hepatic duct, cystic duct, bile dduct, common bile duct, ampula of vater, sphincter of oddi, parts of gall bladder, relation of gall bladder, relation of Common bile duct, complication of bile stone, parts of CBD, blood supply of gall bladder, innervation of gall bladder, blood supply of common bile duct,lymphatic drainage of bile duct and gall bladder
anatomy of duodenum, location or position of duodenum, parts of duodenum, relations of each parts of duodenum, ligaments of treitz, visceral and peritoneal relation of duodenum, blood supply of duodenum, innervation of duodenum, clinical aspects of duodenum, duodenal ulcer, diverticulum, deodinitis, duodenal obstruction
anatomy of spleen, surfaces of spleen, peritoneal an visceral relations, blood supply an lymphatic drainage, hilum of spleen , function of spleen, splenomegaly,
anatomy of spleen, surfaces of spleen, peritoneal an visceral relations, blood supply an lymphatic drainage, hilum of spleen , function of spleen, splenomegaly,
We understand the unique challenges pickleball players face and are committed to helping you stay healthy and active. In this presentation, we’ll explore the three most common pickleball injuries and provide strategies for prevention and treatment.
Navigating the Health Insurance Market_ Understanding Trends and Options.pdfEnterprise Wired
From navigating policy options to staying informed about industry trends, this comprehensive guide explores everything you need to know about the health insurance market.
Defecation
Normal defecation begins with movement in the left colon, moving stool toward the anus. When stool reaches the rectum, the distention causes relaxation of the internal sphincter and an awareness of the need to defecate. At the time of defecation, the external sphincter relaxes, and abdominal muscles contract, increasing intrarectal pressure and forcing the stool out
The Valsalva maneuver exerts pressure to expel faeces through a voluntary contraction of the abdominal muscles while maintaining forced expiration against a closed airway. Patients with cardiovascular disease, glaucoma, increased intracranial pressure, or a new surgical wound are at greater risk for cardiac dysrhythmias and elevated blood pressure with the Valsalva maneuver and need to avoid straining to pass the stool.
Normal defecation is painless, resulting in passage of soft, formed stool
CONSTIPATION
Constipation is a symptom, not a disease. Improper diet, reduced fluid intake, lack of exercise, and certain medications can cause constipation. For example, patients receiving opiates for pain after surgery often require a stool softener or laxative to prevent constipation. The signs of constipation include infrequent bowel movements (less than every 3 days), difficulty passing stools, excessive straining, inability to defecate at will, and hard feaces
IMPACTION
Fecal impaction results from unrelieved constipation. It is a collection of hardened feces wedged in the rectum that a person cannot expel. In cases of severe impaction the mass extends up into the sigmoid colon.
DIARRHEA
Diarrhea is an increase in the number of stools and the passage of liquid, unformed feces. It is associated with disorders affecting digestion, absorption, and secretion in the GI tract. Intestinal contents pass through the small and large intestine too quickly to allow for the usual absorption of fluid and nutrients. Irritation within the colon results in increased mucus secretion. As a result, feces become watery, and the patient is unable to control the urge to defecate. Normally an anal bag is safe and effective in long-term treatment of patients with fecal incontinence at home, in hospice, or in the hospital. Fecal incontinence is expensive and a potentially dangerous condition in terms of contamination and risk of skin ulceration
HEMORRHOIDS
Hemorrhoids are dilated, engorged veins in the lining of the rectum. They are either external or internal.
FLATULENCE
As gas accumulates in the lumen of the intestines, the bowel wall stretches and distends (flatulence). It is a common cause of abdominal fullness, pain, and cramping. Normally intestinal gas escapes through the mouth (belching) or the anus (passing of flatus)
FECAL INCONTINENCE
Fecal incontinence is the inability to control passage of feces and gas from the anus. Incontinence harms a patient’s body image
PREPARATION AND GIVING OF LAXATIVESACCORDING TO POTTER AND PERRY,
An enema is the instillation of a solution into the rectum and sig
Global launch of the Healthy Ageing and Prevention Index 2nd wave – alongside...ILC- UK
The Healthy Ageing and Prevention Index is an online tool created by ILC that ranks countries on six metrics including, life span, health span, work span, income, environmental performance, and happiness. The Index helps us understand how well countries have adapted to longevity and inform decision makers on what must be done to maximise the economic benefits that comes with living well for longer.
Alongside the 77th World Health Assembly in Geneva on 28 May 2024, we launched the second version of our Index, allowing us to track progress and give new insights into what needs to be done to keep populations healthier for longer.
The speakers included:
Professor Orazio Schillaci, Minister of Health, Italy
Dr Hans Groth, Chairman of the Board, World Demographic & Ageing Forum
Professor Ilona Kickbusch, Founder and Chair, Global Health Centre, Geneva Graduate Institute and co-chair, World Health Summit Council
Dr Natasha Azzopardi Muscat, Director, Country Health Policies and Systems Division, World Health Organisation EURO
Dr Marta Lomazzi, Executive Manager, World Federation of Public Health Associations
Dr Shyam Bishen, Head, Centre for Health and Healthcare and Member of the Executive Committee, World Economic Forum
Dr Karin Tegmark Wisell, Director General, Public Health Agency of Sweden
How many patients does case series should have In comparison to case reports.pdfpubrica101
Pubrica’s team of researchers and writers create scientific and medical research articles, which may be important resources for authors and practitioners. Pubrica medical writers assist you in creating and revising the introduction by alerting the reader to gaps in the chosen study subject. Our professionals understand the order in which the hypothesis topic is followed by the broad subject, the issue, and the backdrop.
https://pubrica.com/academy/case-study-or-series/how-many-patients-does-case-series-should-have-in-comparison-to-case-reports/
One of the most developed cities of India, the city of Chennai is the capital of Tamilnadu and many people from different parts of India come here to earn their bread and butter. Being a metropolitan, the city is filled with towering building and beaches but the sad part as with almost every Indian city
1. (lecture 1)
Disclaimer: Presentation is for educational purposes
only and not for commercial activity
Presentedby:
Dr. Archana Rani
Professor
Departmentof Anatomy
KGMU,UP,Lucknow
27.04.2020
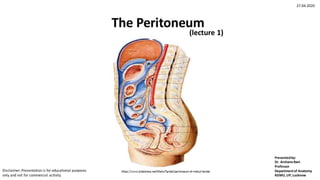
2. Peritoneum
• The peritoneum (Greek stretched over) is a large serous
membrane (serosa) lining the abdominal cavity.
• It is divided into:
a. An outer or parietal layer
b. An inner or visceral layer
c. Folds of peritoneum by which the viscera are suspended
3. Histology of Peritoneum
Histologically, composed
of:
•Outer fibrous layer-
provides strength
•Inner layer of
mesothelial cells-
secrete a serous fluid for
lubrication
https://www.slideshare.net/ahmedsalah925/anatomy-of-peritoneum
4.
5. Diagrammatic transverse section of the abdomen showing the
arrangementof the peritoneum
Human Anatomy. BD Chaurasia, 8th ed, Vol. 2, 2020
6. Parietal Peritoneum
• It lines the inner surface of the
abdominal and pelvic walls
and the lower surface of the
diaphragm.
• Can be easily stripped.
• Derived from somato-pleuric
layer of lateral plate
mesoderm.
• Its blood supply and nerve
supply are the same as those
of the overlying body wall.
• Because of the somatic
innervation, parietal
peritoneum is pain sensitive.
7. Visceral Peritoneum
• It lines the outer surface of the
viscera. In fact it forms a part and
parcel of the viscera.
• Cannot be stripped.
• Derived from splanchno-pleuric
layer of lateral plate mesoderm.
• Its blood supply and nerve supply
are the same as those of the
underlying viscera.
• Because of the autonomic
innervation, visceral peritoneum
evokes pain when viscera is
stretched, ischaemic or distended.
8. Folds of Peritoneum
• Many organs within the abdomen are suspended by folds of
peritoneum. Such organs are mobile.
• Other organs are fixed and immobile. Such organs are said to be
retroperitoneal.
• Some are partially covered.
• Few are sub-peritoneal (infra-peritoneal).
• Provide pathways for passage of vessels, nerves and
lymphatics.
28. CLINICAL ANATOMY
• Ascites: Collection of free fluid in the peritoneal cavity is known as ascites.
Common causes of ascites are cirrhosis of the liver, tubercular peritonitis,
congestive heart failure, and malignant infiltration of the peritoneum. Veins
also get prominent in cirrhosis of liver.
• Peritonitis
• Pneumoperitoneum
• Laparoscopy
• Laparotomy
• Greater omentum limits the spread of infection by sealing off the site of
ruptured vermiform appendix or gastric ulcer and tries to delay the onset of
peritonitis. It is called ‘‘abdominal policeman’’.
• Peritoneal dialysis
34. • Cranial most part forms the
gastrophrenic ligament
https://www.memorangapp.com/flashcards/84729/Abdominal+Wall+and+Peritoneal+Sac+(Lecture+%231
https://anatomyqa.com/stomach-anatomy/
35.
36. Greater Omentum
• The greater omentum (Latin apron) is a large fold of peritoneum which hangs down from the
greater curvature of the stomach like an apron and covers the loops of intestines to a varying
extent.
• Made up of 4 layers.
Contents
• Right and left gastroepiploic vessels
• Fat
Functions
1. It is a storehouse of fat
2. It protects the peritoneal cavity against infection
(collection of macrophages form milky spots)
3. Also known as “policeman of the abdomen”
https://m.youtube.com/watch?v=_bGjvdc5Sqk
39. LESSER OMENTUM
This is a fold of peritoneum which extends from the lesser curvature of the stomach and the
first 2 cm of the duodenum to the liver. The portion of the lesser omentum between the
stomach and the liver is called the hepatogastric ligament, and the portion between the
duodenum and the liver is called the hepatoduodenal ligament.
Attachments:
Inferiorly: lesser curvature of stomach and duodenum
Superiorly: liver in the form of an inverted ‘L’
Contents:
The right free margin of the lesser omentum contains:
1. The proper hepatic artery
2. The portal vein
3. The bile duct
4. Lymph nodes & lymphatics
5. Hepatic plexus of nerves
40. The attachments and contents of the lesser omentum. The liver has been
turned upwards so that its posteroinferior surface can be seen
41. MESENTERY
The mesentery (Greek fold of intestine) of the small intestine or
mesentery proper is a broad, fan-shaped fold of peritoneum
which suspends the coils of jejunum and ileum from the posterior
abdominal wall.
https://www.kenhub.com/en/library/anatomy/mesentery
42. Borders
• The attached border, or root of the
mesentery, is 15 cm long, it crosses the
following structures:
1.The third part of the duodenum
where the superior mesenteric
vessels enter into it
2.The abdominal aorta
3.The inferior vena cava
4.The right ureter
5.The right psoas major
• Free or intestinal border is 6 metres long.
• The breadth of the mesentery is
maximum and is about 20 cm in the
central part, but gradually diminishes
towards both the ends.
https://www.kenhub.com/en/library/anatomy/mesentery
43. Contents
1. Jejunal and ileal branches of the superior mesenteric artery
2. Accompanying veins
3. Autonomic nerve plexuses
4. Lymphatics or lacteals
5. 100–200 lymph nodes
6. Connective tissue with fat
https://www.slideshare.net/DrSherifFahmy/jejunum-ileum-anatomy-of-the-abdomen
44. Mesoappendix
It is a small, triangular fold of peritoneum which
suspends the vermiform appendix from the posterior
surface of the lower end of the mesentery close to the
ileocaecal junction.
45. Transverse Mesocolon
Attachments
• The root of the transverse
mesocolon is attached to the
anterior surface of the head, and
the anterior border of the body of
the pancreas.
Contents
• It contains the middle colic vessels;
the nerves, lymph nodes and
lymphatics of the transverse colon.
https://www.memorangapp.com/flashcards/71585/Inferior+Mesenteric+Artery+and+Large+intestine/
46. Sigmoid Mesocolon
Features
• This is a triangular (Greek ‘S’ shape)
fold of peritoneum which suspends
the sigmoid colon from the pelvic wall.
Attachments
• The root is shaped like an inverted ‘V’.
Contents
• The sigmoid vessels in the left limb;
superior rectal vessels, nerves, lymph
nodes and lymphatics in the right limb
of the sigmoid colon.