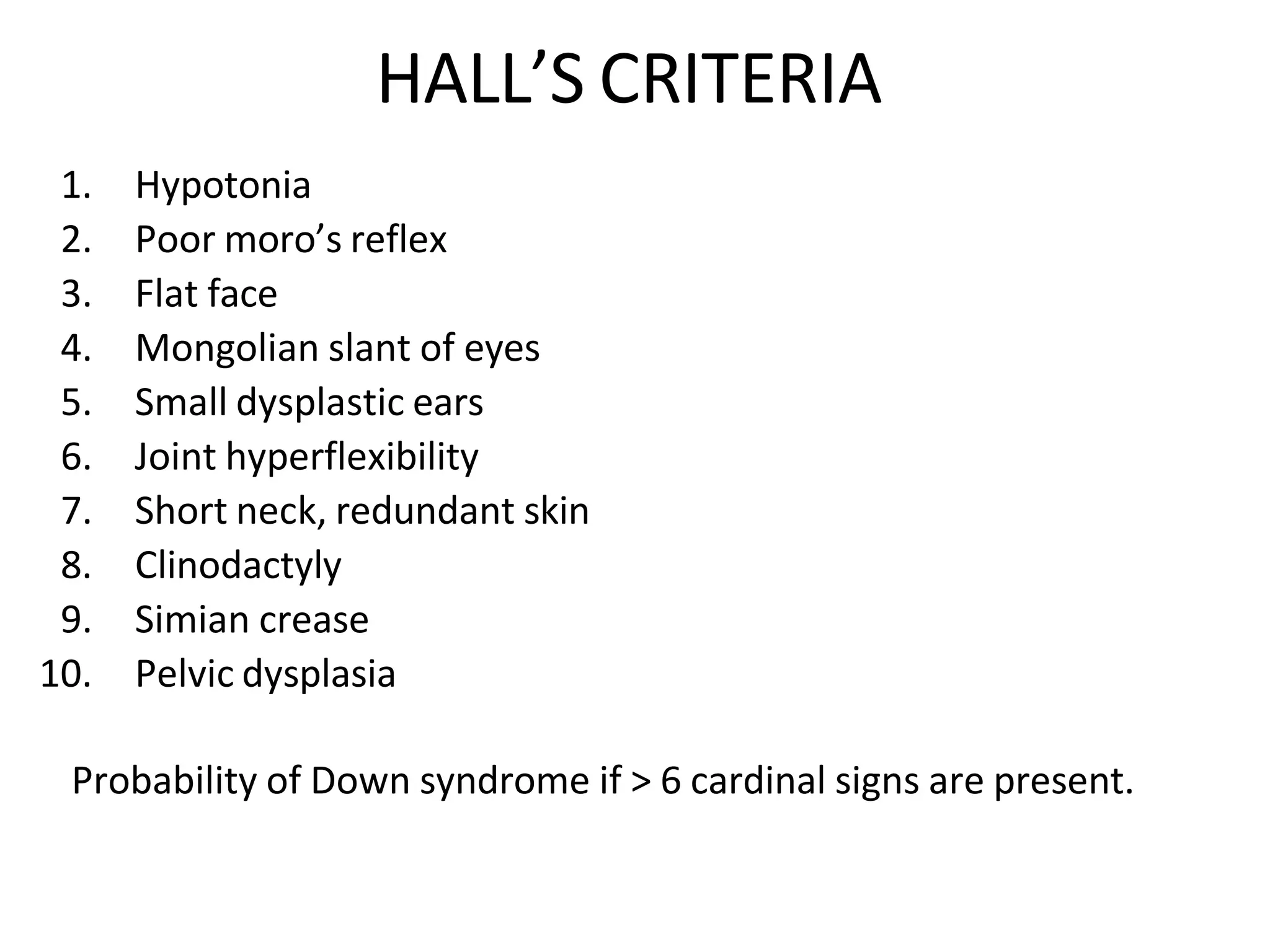
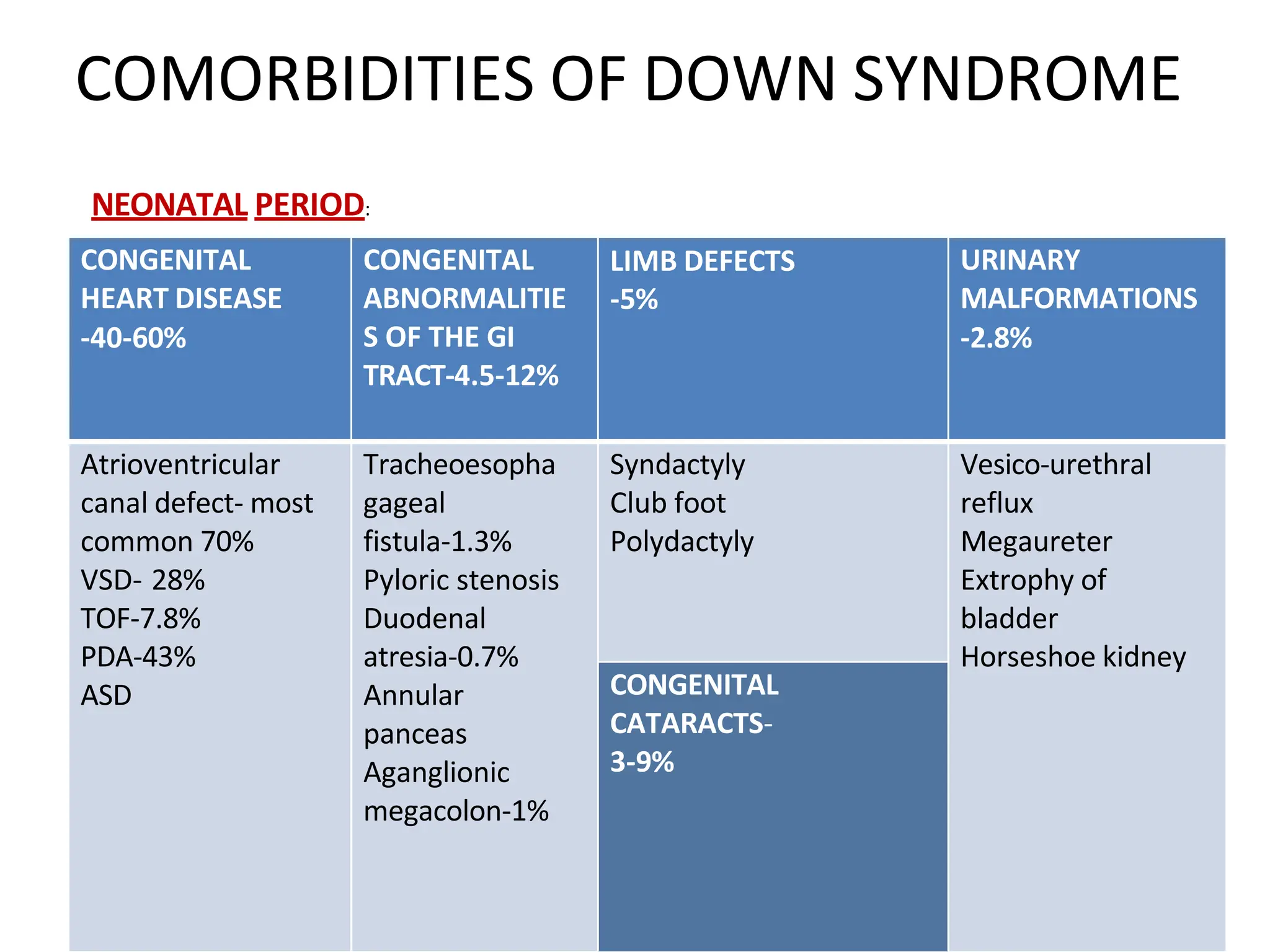
Down syndrome, caused by trisomy 21, affects approximately 1 in 733 live births, with a higher incidence in India. Characterized by features such as hypotonia, flat facial profile, and various congenital comorbidities, early diagnosis through karyotype analysis and phenotypic assessment is crucial for management. Advancements in therapies and support systems have significantly improved life expectancy and quality of life for individuals with Down syndrome.