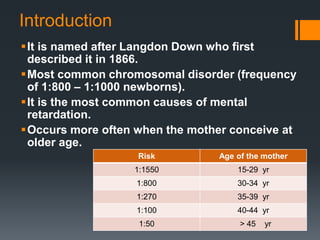
Down syndrome, first described by Langdon Down in 1866, is the most common chromosomal disorder affecting 1 in 800 to 1 in 1000 newborns and is often linked to older maternal age. This disorder is primarily caused by meiotic non-disjunction of chromosome 21, with various clinical features including mental and physical retardation, distinct facial characteristics, and associated health issues such as congenital heart disease and hypothyroidism. Early diagnosis and management, including physiotherapy and counseling for parents, are essential for improving outcomes and development.












































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














