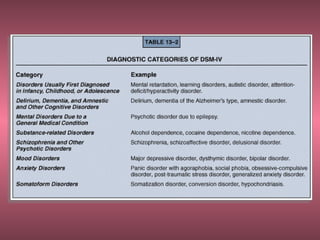
The document discusses perspectives on psychological disorders from society, individuals, and mental health professionals. It then covers various approaches to understanding disorders, including biological, psychoanalytic, cognitive-behavioral, and diathesis-stress models. It provides an overview of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV), which classifies over 230 psychological disorders into 16 categories. Specific categories and disorders discussed include mood disorders like depression and bipolar disorder, anxiety disorders like phobias and obsessive-compulsive disorder, and somatoform disorders. Causes of disorders are explored from biological, psychological, and social perspectives.