This document discusses disorders of the adrenal cortex. It begins by outlining the learning objectives, which are to understand the etiology, pathophysiology, clinical manifestations, diagnostics, treatment, nursing care, and complications of adrenal cortex disorders. It then provides an overview of adrenal gland disorders in general before focusing specifically on the adrenal cortex and its hormones. Key points covered include the causes, symptoms, diagnostic tests, and treatment of adrenal hypofunction conditions like Addison's disease and adrenal hyperfunction conditions.
The adrenal cortex produces three major classes of steroids:
glucocorticoids,
(2) mineralocorticoids, and
(3) adrenal androgens.
Consequently, normal adrenal function is important for
-modulating intermediary metabolism and immune responses through glucocorticoids;
blood pressure, vascular volume, and electrolytes through mineralocorticoids;
secondary sexual characteristics (in females) through androgens.
The adrenal axis plays an important role in the stress response by rapidly increasing cortisol levels.
Adrenal disorders include hyperfunction (Cushing's syndrome) and hypofunction (adrenal insufficiency) as well as a variety of genetic abnormalities of steroidogenesis.
The adrenal cortex produces three major classes of steroids:
glucocorticoids,
(2) mineralocorticoids, and
(3) adrenal androgens.
Consequently, normal adrenal function is important for
-modulating intermediary metabolism and immune responses through glucocorticoids;
blood pressure, vascular volume, and electrolytes through mineralocorticoids;
secondary sexual characteristics (in females) through androgens.
The adrenal axis plays an important role in the stress response by rapidly increasing cortisol levels.
Adrenal disorders include hyperfunction (Cushing's syndrome) and hypofunction (adrenal insufficiency) as well as a variety of genetic abnormalities of steroidogenesis.
This lecture talk about the disturbance of adrenal gland hormones and how it affect health. it also discuss in brief how to manage such condition in your dental clinic
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
Knee anatomy and clinical tests 2024.pdfvimalpl1234
This includes all relevant anatomy and clinical tests compiled from standard textbooks, Campbell,netter etc..It is comprehensive and best suited for orthopaedicians and orthopaedic residents.
New Drug Discovery and Development .....NEHA GUPTA
The "New Drug Discovery and Development" process involves the identification, design, testing, and manufacturing of novel pharmaceutical compounds with the aim of introducing new and improved treatments for various medical conditions. This comprehensive endeavor encompasses various stages, including target identification, preclinical studies, clinical trials, regulatory approval, and post-market surveillance. It involves multidisciplinary collaboration among scientists, researchers, clinicians, regulatory experts, and pharmaceutical companies to bring innovative therapies to market and address unmet medical needs.
Prix Galien International 2024 Forum ProgramLevi Shapiro
June 20, 2024, Prix Galien International and Jerusalem Ethics Forum in ROME. Detailed agenda including panels:
- ADVANCES IN CARDIOLOGY: A NEW PARADIGM IS COMING
- WOMEN’S HEALTH: FERTILITY PRESERVATION
- WHAT’S NEW IN THE TREATMENT OF INFECTIOUS,
ONCOLOGICAL AND INFLAMMATORY SKIN DISEASES?
- ARTIFICIAL INTELLIGENCE AND ETHICS
- GENE THERAPY
- BEYOND BORDERS: GLOBAL INITIATIVES FOR DEMOCRATIZING LIFE SCIENCE TECHNOLOGIES AND PROMOTING ACCESS TO HEALTHCARE
- ETHICAL CHALLENGES IN LIFE SCIENCES
- Prix Galien International Awards Ceremony
Acute scrotum is a general term referring to an emergency condition affecting the contents or the wall of the scrotum.
There are a number of conditions that present acutely, predominantly with pain and/or swelling
A careful and detailed history and examination, and in some cases, investigations allow differentiation between these diagnoses. A prompt diagnosis is essential as the patient may require urgent surgical intervention
Testicular torsion refers to twisting of the spermatic cord, causing ischaemia of the testicle.
Testicular torsion results from inadequate fixation of the testis to the tunica vaginalis producing ischemia from reduced arterial inflow and venous outflow obstruction.
The prevalence of testicular torsion in adult patients hospitalized with acute scrotal pain is approximately 25 to 50 percent
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
Flu Vaccine Alert in Bangalore Karnatakaaddon Scans
As flu season approaches, health officials in Bangalore, Karnataka, are urging residents to get their flu vaccinations. The seasonal flu, while common, can lead to severe health complications, particularly for vulnerable populations such as young children, the elderly, and those with underlying health conditions.
Dr. Vidisha Kumari, a leading epidemiologist in Bangalore, emphasizes the importance of getting vaccinated. "The flu vaccine is our best defense against the influenza virus. It not only protects individuals but also helps prevent the spread of the virus in our communities," he says.
This year, the flu season is expected to coincide with a potential increase in other respiratory illnesses. The Karnataka Health Department has launched an awareness campaign highlighting the significance of flu vaccinations. They have set up multiple vaccination centers across Bangalore, making it convenient for residents to receive their shots.
To encourage widespread vaccination, the government is also collaborating with local schools, workplaces, and community centers to facilitate vaccination drives. Special attention is being given to ensuring that the vaccine is accessible to all, including marginalized communities who may have limited access to healthcare.
Residents are reminded that the flu vaccine is safe and effective. Common side effects are mild and may include soreness at the injection site, mild fever, or muscle aches. These side effects are generally short-lived and far less severe than the flu itself.
Healthcare providers are also stressing the importance of continuing COVID-19 precautions. Wearing masks, practicing good hand hygiene, and maintaining social distancing are still crucial, especially in crowded places.
Protect yourself and your loved ones by getting vaccinated. Together, we can help keep Bangalore healthy and safe this flu season. For more information on vaccination centers and schedules, residents can visit the Karnataka Health Department’s official website or follow their social media pages.
Stay informed, stay safe, and get your flu shot today!
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
micro teaching on communication m.sc nursing.pdfAnurag Sharma
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
Recomendações da OMS sobre cuidados maternos e neonatais para uma experiência pós-natal positiva.
Em consonância com os ODS – Objetivos do Desenvolvimento Sustentável e a Estratégia Global para a Saúde das Mulheres, Crianças e Adolescentes, e aplicando uma abordagem baseada nos direitos humanos, os esforços de cuidados pós-natais devem expandir-se para além da cobertura e da simples sobrevivência, de modo a incluir cuidados de qualidade.
Estas diretrizes visam melhorar a qualidade dos cuidados pós-natais essenciais e de rotina prestados às mulheres e aos recém-nascidos, com o objetivo final de melhorar a saúde e o bem-estar materno e neonatal.
Uma “experiência pós-natal positiva” é um resultado importante para todas as mulheres que dão à luz e para os seus recém-nascidos, estabelecendo as bases para a melhoria da saúde e do bem-estar a curto e longo prazo. Uma experiência pós-natal positiva é definida como aquela em que as mulheres, pessoas que gestam, os recém-nascidos, os casais, os pais, os cuidadores e as famílias recebem informação consistente, garantia e apoio de profissionais de saúde motivados; e onde um sistema de saúde flexível e com recursos reconheça as necessidades das mulheres e dos bebês e respeite o seu contexto cultural.
Estas diretrizes consolidadas apresentam algumas recomendações novas e já bem fundamentadas sobre cuidados pós-natais de rotina para mulheres e neonatos que recebem cuidados no pós-parto em unidades de saúde ou na comunidade, independentemente dos recursos disponíveis.
É fornecido um conjunto abrangente de recomendações para cuidados durante o período puerperal, com ênfase nos cuidados essenciais que todas as mulheres e recém-nascidos devem receber, e com a devida atenção à qualidade dos cuidados; isto é, a entrega e a experiência do cuidado recebido. Estas diretrizes atualizam e ampliam as recomendações da OMS de 2014 sobre cuidados pós-natais da mãe e do recém-nascido e complementam as atuais diretrizes da OMS sobre a gestão de complicações pós-natais.
O estabelecimento da amamentação e o manejo das principais intercorrências é contemplada.
Recomendamos muito.
Vamos discutir essas recomendações no nosso curso de pós-graduação em Aleitamento no Instituto Ciclos.
Esta publicação só está disponível em inglês até o momento.
Prof. Marcus Renato de Carvalho
www.agostodourado.com
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
2. LEARNING OBJECTIVE
At the end of this session,
I. Student are able to understand etiology and
pathophysiology of adrenal cortex disorder
II. Identify the clinical manifestation
III. Explain the diagnostic investigation related
IV. Discuss the treatment, intervention and
possible complication
V. Apply nursing art / caring value towards
patient ~ nursing care
3. OVERVIEW OF ADRENAL GLANDS
DISORDER
It’s condition that interfere with the normal
function of the adrenal glands
It may cause hyperfunction or hypofunction, and
may be congenital or acquired
Function of adrenal glands
produces hormones that affect growth
Development and stress
Helps in regulate kidney function
Consist of 2 parts
adrenal cortex
Adrenal medulla
Both parts are structurally and
functionally different
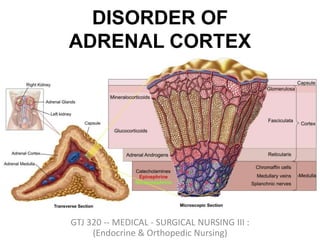
5. ADRENAL CORTEX
I. Outer part of gland
Part of hypothalamus – pituitary – adrenal axis
II. Secrete a variety of steriodhormones
mineralocorticoids : regulate salt and water
balance within the body
Glucocorticoids (include cortisol) : wide
number of roles within the body
Androgens : hormones with testosterone
like function
6. ADRENAL MEDULLA
I. Inner part of gland (20% of gland)
Part of sympathetic nervous system
2. Secrete catecholamine's
Epinephrine
Norepinephrine
7.
8. Primary
Regulatory Control
Anatomy Secretory products
Renin-angiotensin Zona
glomerulosa
Aldosterone
ACTH,
hypothalamic CRH
Zona fasciculata Cortisol and sex
hormones
ACTH,
hypothalamic CRH
Zona reticularis Sex hormones (e.g.
androgens)
Preganglionic
sympathetic fibers
Medulla Catecholamines (Epi,
NE)
9. ADRENAL CIRCULATION
• Both the left and right adrenals receive arterial blood
supply in the same fashion
• Paired superior suprarenal arteries - derived from inferior
phrenic arteries
• Paired middle suprarenal arteries - derived directly from
abdominal aorta
• Paired inferior suprarenal arteries - derived from the adjacent
renal arteries
• The left and right adrenals have differing venous
drainage
• The left adrenal venous drainage is through the left adrenal
vein to the left renal vein and finally to the IVC
• The right adrenal venous drainage is through the right
adrenal vein to the IVC
• Recall the same pattern for the left and right gonadal
artery/vein
10. HISTOLOGY OF ADRENAL GLANDS
Adrenal cortex : Arranged in zonal configuration
Outer zona glomerulosa = small, compact cells
Central zona fasciculata = larger, lipid-rich cells
arranged in radial columns
Inner zona reticularis = compact & pigmented cells
Adrenal medulla
Thin layers of large chromaffin cells
15. ADRENAL CORTEX
• Thelarge cortical cells are arranged into three
layers or zones:
– Thezona glomerulosa,
• Thethin outermost layer
• Constitute about 15%of cortex
– Thezona fasciculata,
• Themiddle and largest portion
• Constitute about 75%of cortex.
– Thezona reticularis,
• Theinnermost zone
16. ADRENAL CORTEX
• Zonaglomerulosa:
– Produce meniralocorticods
– Mainly aldosterone (because it containenzyme
aldosterone synthase)
•Hormones that help control the balance of
minerals (Na+ and K+)and water in theblood
19. ADRENAL CORTEX
• Zonafasciculata:
– Produce glucocorticods
– Mainly cortisol andcorticosterone
– Thehuman adrenal glands produce the equivalent
of 35–40 mg of cortisone acetate perday
Hormone that play amajor role inglucose
metabolism aswell asin protein and lipid
metabolism
– Thesecretion of these cells is controledby
hypothalamic-pituitary axis viaACTH
20. ADRENAL CORTEX
• Zonareticularis:
– Theinnermost layer of the adrenal cortex, lying
deep to the zonafaciculata and superficial tothe
medulla.
– Thesecells produce androgens
21. ADRENAL CORTEX
• Zonareticularis:
–Theandrogens produced includes
• Dehydroepiandrosterone (DHEA)
• Androstenedione
– Synthesized from cholesterol
• DHEAis further converted to DHEA-
sulfate viaa sulfotransferase
22. ADRENAL CORTEX
• Zonareticularis:
– Theandrogens produced are released into the
blood stream and taken up in the testis and
ovaries to produce testosterone and theestrogens
respectively.
23. DISORDER OF ADRENAL CORTEX
• Patient with adrenal disorders canpresent
with features relatedto:
• HYPOFUNCTIONOFTHEGLAND
• HYPERFUNCTIONOFTHEGLAND
26. INTRODUCTION OF ADRENAL
HYPOFUNCTION
Its a condition in which the adrenal glands are
unable to perform well or function less than what
they normally should.
The causes of adrenal hypofunction are many and
include a variety of factors including autoimmune
disease.
The symptoms of adrenal hypofunction need to
be understood well to be able to diagnose and
manage the condition.
Treatment of adrenal hypofunction is mainly
based on its causes and symptoms.
27. ADRENAL HYPOFUNCTION
• Adrenal insufficiency leads to a reduction in
the output of adrenal hormones
– glucocorticoids and/or mineralocorticoids
• Twotypesof adrenalinsufficiency
• Primaryinsufficiency/ Adrenal hypofunction
• inability of the adrenal glandstoproduce enough
steroid hormones
• Secondaryinsufficiency/ Adrenal hypofunction
• inadequate pituitary or hypothalamic stimulation of
the adrenal glands
28. CAUSES OF PRIMARY ADRENAL
HYPOFUNCTION
Autoimmune disease
Genetic diseases
Infections
Bleeding in glands
Surgical removal of adrenal glands
29. CAUSES OF SECONDARY ADRENAL
HYPOFUNCTION
Condition affecting the pituitary gland can cause
secondary adrenal hypofunction.
The pituitary glands are liable for producing a
hormone which conveys message to adrenal gland to
produce required cortisol for bodily functioning.
If the pituitary gland fails to do this, then no more
cortisol will be produced and this causes secondary
adrenal hypofunction.
31. OTHERS CAUSES OF ADRENAL
HYPOFUNCTION
Metabolic failure in hormone production
•Congenital adrenal hyperplasia e.g. 21-
hydroxylase deficiency, 3-β-hydroxysteroid
dehydrogenase deficiency
•Enzyme inhibition e.g. ketoconazole
•Accelerated hepatic metabolism of cortisol
e.g. phenytoin, barbiturates, rifampicin
33. SYMPTOMS OF ADRENAL
HYPOFUNCTION
Symptoms of adrenal hypofunction mostly
based on the deficiency of hormone
aldosterone & cortisol
High / low blood pressure
Low blood sugar level
Craving for salty foods
Excessive sweating
34. SYMPTOMS OF ADRENAL
HYPOFUNCTION
Unnecessary weight loss
Fatigue that becomes worse with passing days
Loss of appetite
Muscle weakness
Irregular or no menstruation in females
Headaches.
35. ROLES OF HORMONE
ALDOSTERONE & CORTISOL
To maintain immune system
To regulate blood pressure and blood glucose
level
To maintain salt and electrolytes balance in
the body
To ensure heart muscles tone and healthy
bones
To increase body's response to stress.
36. LAB TEST FOR ADRENAL
HYPOFUNCTION
Serum level of cortisol, adrenocorticotropic
hormone (ACTH) and Corticotropin-releasing
hormone (CRH)
ACTH& CRH stimulation test (more specific)
X-ray
Ultrasound
MRI / Ct Scan
Detect any changes /
problems in adrenal
glands or pituitary glands
37. TREATMENT FOR ADRENAL
HYPOFUNCTION
Cortisol replacement steroids therapy
Oral replacement (based on height , weight
and medication used)
Injections (for serious symptoms or adrenal
crisis
o Only prescribed for emergency
situations
Specialized diet
39. WHAT IS ADDISON’S DISEASE
Addison's disease is a disorder that occurs
when body produces insufficient amounts of
cortisol and often insufficient levels of
aldosterone as well.
Also called adrenal insufficiency, Addison's
disease occurs in all age groups and affects
both sexes.
Addison's disease can be life-threatening.
41. SYMPTOMS OF ADDISON’S
DISEASE
Extreme fatigue
Weight loss & appetite
Darkening of your skin
(hyperpigmentation)
Low blood pressure, even
fainting
Salt craving
Hypoglycemia
• Nausea, diarrhea or
vomiting
• Abdominal pain
• Muscle or joint pains
• Irritability
• Depression
• Body hair loss or sexual
dysfunction in women
Usually develop slowly , often over several months
47. ADDISON’S DISEASE : TREATMENT
Two main treatment
1. Oral corticosteroids
Hydrocortisone (Cortef), prednisone or cortisone
acetate may be used to replace cortisol. Your
doctor may prescribe fludrocortisone to replace
aldosterone.
2. Corticosteroid injection
For those not intolerant with oral
48. ADDISON’S DISEASE : TREATMENT
Replacement of hormones
glucocorticoid : hydrocortisone 15mg on waking
and 5mg at night
Mineralocorticoid : fludrocortisone 0.05mg to 0.1
mg daily
Supportive treatment & treatment causes
if TB : anti-tubercular therapy
49. ADDISON’S DISEASE : TREATMENT
General advice to the patient
good nutrition : regular meal,
high carbohydrate : prevent weight gain
sufficient salt : minimize edema and reduce risk for
hypertension
Diabetic diet : glucose intolerant
Administer with meal to prevent ulcer ; When oral
therapy is not possible, injection hydrocortisone
should be taken.
Provide supplementary potassium if possible
55. ADDISONIAN CRISIS : CAUSES
Sudden withdrawal of steroid(commonest cause, if pt.
on steroid for long time)
Following stress e.g.intercurrent disease,trauma,
surgery, severe infection or prolonged fasting in a pt
with latent insufficiency
Following sudden destruction of pituitary
gland(pituitary necrosis)or when thyroid hormone or
drugs which increase steroid metabolism(e.g.
phenytoin)given to a pt with hypoadrenalism
Following bilateral adrenalectomy
Following injury to both adrenals due to
trauma,adrenal vein thrombosis,adrenal haemorrhage
due to meningococcaemia or anticoagulant therapy
57. ADDISONIAN CRISIS : TREATMENT
I/V hydrocortisone 100 mg 6 hrly until GI
symptoms abate then oral therapy
I/V fluid normal saline and 10% dextrose for
hypoglycaemia
Precipitating factors should be find out and
treated
58.
59.
60.
61. ADDISONIAN CRISIS : DEATH
Common causes for death is when patient
developed an acute adrenocortical
insufficiency and died ~ integrated with other
medical problems as example patient may
have subclinical hypoadrenalism – increased
hepatic metabolism by drug induced
63. ADDISON’S DISEASE : NURSING
INTERVENTIONS
2. Coping and support
3. Maintain with follow up / appointment with
physician
4. Health education : noted symptoms, make a
list of medication, inform family members
65. ADRENAL HYPERFUNCTION
• It is a condition where there is an
overexpression / excessive production of one
or more adrenal hormones (aldosterone,
corticosteroids, androgenic steroids,
epinephrine and norepinephrine).
• The increased adrenal gland activity may be
caused by an adrenal gland tumor or by
excessive stimulation of the gland. Pituitary
hormones stimulate adrenal gland activity.
66. ADRENAL HYPERFUNCTION
There are 3 basic types of corticosteroids
elaborated by the adrenal cortex “
glucocorticoids, mineralocorticoids, and sex
hormone ” and 4 distinctive hyperadrenal
clinical sydromes:
• Cushing syndrome : “ excess cortisol ”
• Hyperaldosteronism : “ excess aldestrone”
• Adrenogenital syndromes : “excess androgen”
• Pheochromocytoma : “ high catecholamine”
67. HYPERALDOSTERONISM
• A medical condition where too much
aldosterone is produced by the adrenal
glands, which can lead to sodium retention
and potassium loss.
• Types:
–Primary hyperaldosteronism
–Secondary hyperaldosteronism
69. PRIMARY HYPERALDOSTERONISM
/ CONN’S SYNDROME
1. Characterized by autonomous excessive
production of aldosterone by adrenal glands
2. Presents with hypertension , hypokalaemic
alkalosis and renal K+ wasting
70. PRIMARY HYPERALDOSTERONISM
/ CONN’S SYNDROME
• Causes:
– Adrenal adenoma
– Bilateral hypertrophy of zona glomerulosa
cells
– Adrenal carcinoma
•Rare cause
71. PRIMARY HYPERALDOSTERONISM
/ CONN’S SYNDROME
• Clinical features:
– Hypertension : aldosterone induced Na
retention with increase in Extra cellular
fluid volume
– Muscle weakness: Due to decrease K+
– Muscle paralysis: severe hypokalaemia
– Latent tetany (continuous tonic spasm of a
muscle; )and paraesthesiae (numbness,
itching, and a feeling of pins and needles on
your skin)
– Polydipsia, polyuria and nocturia: due to
hypokalaemic nephropathy
73. PRIMARY HYPERALDOSTERONISM
/ CONN’S SYNDROME
Investigation
• Plasma aldosterone : renin activity ratio
– Sensitive screening test
– No need to standardize posture
Ratio Interpretation Action
<800 Diagnosis excluded Seek other cause
>1000,<2000 Diagnosis possible Confirmatory test
>2000 Diagnosis very likely Establish cause
74. SECONDARY ALDOSTERONISM
• Is increased adrenal production of aldosterone
in response to non-pituitary, extra-adrenal
stimuli
• Increase renin secretion
– (hyperreninemic hyperaldosteronism)
• Commoner than primary aldosteronism
75. SECONDARY ALDOSTERONISM
Common
• CCF
• Liver cirrhosis with
ascities
• Nephrotic syndrome
Less common
• Renal artery stenosis
• Sodium – losing
nephritis
• Renin—secreting
tumours
76. CUSHING’S SYNDROME
• Adrenal cortex hyperfunction
• Any condition resulting from overproduction
of primarily glucocorticoid (cortisol)
• Mineralocorticoid and androgen may also be
excessive
77.
78. CAUSES OF CUSHING’S SYNDROME
1. External versus Internal
o effect of corticosteroid treatment
o asthma and rheumatoid arthritis, or in
immunosuppression after an organ transplant.
o Over use of medroxyprogesterone acetate
2. Pseudo-Cushing's syndrome
79. PSEUDO - CUSHING’S SYNDROME
• Appear cushingoid and have some
biochemical abnormalities of true
Cushing’s disease
• Causes
– Severe depression
– Alcoholism
– Obesity
– Polycystic ovarian syndrome
87. PSEUDO - CUSHING’S SYNDROME
: CLINICAL FEATURES
• Back pain ( osteoporosis and vertebral
collapse) – inhibit bone formation
• Psychiatric disturbances – euphoria,
mania, depression
88.
89. PSEUDO - CUSHING’S SYNDROME :
LABORATORY INVESTIGATIONS
There are two diagnostic steps in the
investigation of patient suspected of having
Cushing's syndrome
Screening test
for identification of Cushing's syndrome.
the demonstration of high plasma cortisol
level
Identification of cause
90. PSEUDO / CUSHING’S SYNDROME :
LABORATORY INVESTIGATIONS
1. Assessment of circadian rhythm in cortisol
secretion.
Measure 8 am and 11 pm serum cortisol
level
Normal : Serum value @ midnight is 50%
less than value @ 8 am
Cushing’s syndrome : rhythum is loss
Pseudo-Cushing : normal circadian.
91. PSEUDO / CUSHING’S SYNDROME :
LABORATORY INVESTIGATIONS
2. Measuring 24-hour urinary free cortisol
Level (umol /24 h Interpretation
< 300 Normal
300 - 700 Severe depression
Stress
> 700 Diagnostic of Cushing’s
syndrome
92. PSEUDO / CUSHING’S SYNDROME :
LABORATORY INVESTIGATIONS
3. Low dose Dexamethasone suppression test :
0.5 mg Dexametason (oral) given 6 hourly for 2
days
blood for plasma cortisol collected 6 hour after
last dose
urine for urine free cortisol test(UFC) is
collected before & on the 2nd day of Dexa
93. PSEUDO / CUSHING’S SYNDROME :
LABORATORY INVESTIGATIONS
3. Low dose Dexamethasone suppression test :
RESULT
UFC suppress by 50% ( < 70nmol/24h Normal
plasma cortisol suppress < 140 nmol/L
Cushing
Pseudo CS
no suppression of UFC & Pl. cortisol Cushing’s
Syndrome
94. PSEUDO / CUSHING’S SYNDROME :
LABORATORY INVESTIGATIONS
4. High dose Dexamethasone suppression test :
• Normal individuals suppress plasma cortisol
to < 50 nmol/L.
• Patients with Cushing's syndrome fail to show
complete suppression of plasma cortisol
levels. This test is highly sensitive (> 97%).
96. PSEUDO / CUSHING’S SYNDROME :
LABORATORY INVESTIGATIONS
6. Corticotrophin-releasing hormone (CRH )Test
Differentiate ectopic ACTH secretion and
Cushing’s disease.
Cushing’s disease – plasma ACTH increases
50% over baseline & cortisol increase by 20%
Ectopic ACTH or adrenal tumour – no response
97. PSEUDO / CUSHING’S SYNDROME :
LABORATORY INVESTIGATIONS
7. Imaging
CT scan of adrenal gland:TRO adrenal tumor
MRI of pituitary gland: majority microadenoma
( < 10mm). MRI reveal lesion in 50 - 60% of
cases
CT scan/MRI of thorax & abdomen: ectopic
ACTH producing tumor
98. PSEUDO / CUSHING’S SYNDROME :
TREATMENT
• Depend of Cushing's syndrome depends on
the etiology:
– Adrenal adenoma
– Adrenal Carcinoma – resection
– Cushing’s disease - transphenoidal hyposectomy
– Drug ( block cortisol synthesis ) - metyrapone
99.
100. PHEOCHROMOCYTOMA
• Pheochromocytoma is an extremely rare pathological
condition of the adrenal glands where there is
development of benign tumors on the cells present in
the center of the gland causing symptoms.
• The adrenal glands are located at the top of each
kidney and are responsible for producing hormones
which provide instructions to all the organs and tissues
of the body.
101. PHEOCHROMOCYTOMA : CAUSES
• It’s normally develops in the specialized cells
of the adrenal gland called the chromaffin
cells.
• These cells are located right in the center of
the adrenal gland and are responsible for
secreting hormones primarily adrenaline.
• The hormone adrenaline comes to play when
an individual is under stress and calms the
body down.
102. PHEOCHROMOCYTOMA : CAUSES
• This hormone results in an individual having
higher blood pressure readings and a fast
heart rate.
• Pheochromocytoma can causes irregular and
excessive release of adrenaline.
• Rare but treatable
103. PHEOCHROMOCYTOMA : RISK
FACTOR
• Multiple Endocrine Neoplasia - Type II: This is a disorder in
which there is development of tumors in the endocrine
system of the body including the thyroid, parathyroid, lips,
tongue and the gastrointestinal tract.
• Von Hippel-Lindau Disease: This disease can result in
development of tumor in the central nervous system,
endocrine system, pancreas, and kidneys.
• Neurofibromatosis-1: This condition results in
development of tumor in the skin and the optic nerve.
104. PHEOCHROMOCYTOMA :
SYMPTOMS
• Some of the most common symptoms of are:
–Persistent high blood pressure
–Persistent rapid heartbeat
–Excessive sweating
–Severe / persistent headaches
–Tremors
–Having a pale face
–Shortness of breath.
105. PHEOCHROMOCYTOMA :
SYMPTOMS
• Some of the less common symptoms of are:
–Severe anxiety
–Abdominal pain
–Constipation
–Unintentional weight loss.
108. PHEOCHROMOCYTOMA :
COMPLICATIONS
1- Hormone function:
• ECG, ECHO, and blood glucose level.
• Suppressor test: clonidine injection iv 5mg
→ ↓ of BP by 53/25 mmhg for 15 minutes
Due to blockade of alpha-receptors in other
forms of hypertension but not in
Pheochromocytoma.
109. PHEOCHROMOCYTOMA :
COMPLICATIONS
2- Hormone level:
serum catecholamines level is elevated
(n=2-5mg/L)
neurophysin serum level is elevated
(secreted in equimolar concentration with
epinephrine)
110. PHEOCHROMOCYTOMA :
COMPLICATIONS
3. Hormone end product:
24hrs urinary vallinyl mandelic acid (VMA)
is elevated
Should be collected in acidic medium and
refrigerated).
The result of the test is falsely high
In patients taking alpha-methyl dopa,
banana or pine apple (n=2-6 mg/24 hrs).
111. PHEOCHROMOCYTOMA :
COMPLICATIONS
4- Cause:
CT, MRI or sonography of abdomen
iodine 131 -metaiodobenzyl guanidine (MIBG)
scanning, particularly in extra-abdominal
Tumors.
Intravenous pyelogram (IVP) may show
indentation of the upper pole of kidney
112.
113. PHEOCHROMOCYTOMA :
TREATMENT
• Surgical removal of tumour
• Calcium channel blockers control BP
• Sympathetic blocking agents
– Reduce blood pressure
– Reduce symptoms of catecholamine excess
• Beta blockers to reduce dysrhythmias
• Monitor blood sugar/glucose level
114. SUMMARY
• The adrenal glands are small glands located on top of
each kidney and produce hormones that can't live
without, including sex hormones and cortisol.
• In adrenal gland disorders, glands make too much or
not enough hormones. In Cushing's syndrome, there's
too much cortisol, while with Addison's disease, there
is too little. Some people are born unable to make
enough cortisol.