
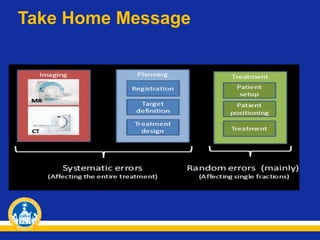
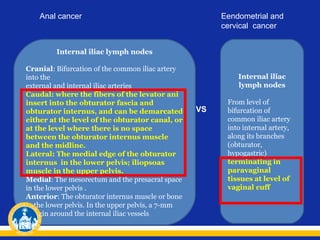
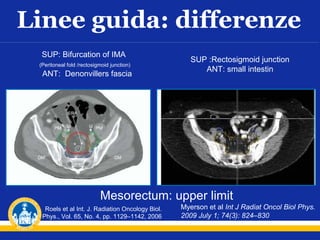


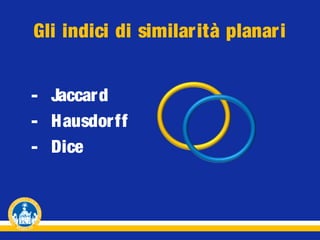









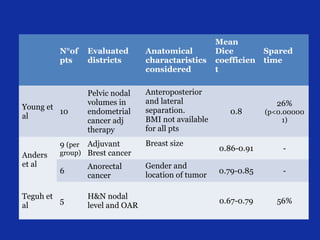
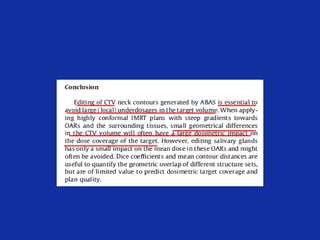

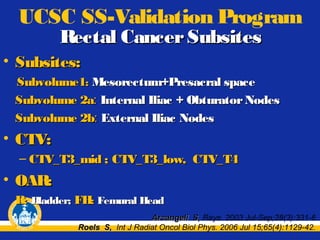
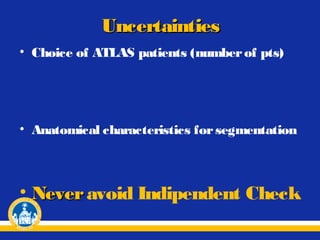
![N°of
pts
Evaluated
districts
Anatomical
charactaristics
considered
10
Pelvic nodal
volumes in
endometrial
cancer adj
therapy
Anteroposterior
and lateral
separation.
BMI not available
for all pts
9 (per
Adjuvant
Brest cancer
Breast size
6
Anorectal
cancer
Gender and
location of tumor
5
H&N nodal
level and OAR
Young et al,
Int. J. Radiation
Oncology Biol.
Phys., Vol. 79, No. 3,
pp. 943–947, 2011
Anders et al,
Radiotherapy and
Oncology 102
(2012) 68–73
group)
Teguh et al,
Int. J. Radiation
Oncology Biol. Phys.,
Vol. 81, No. 4, pp.
950–957, 2011
Gambacorta
et al,
10
Acta Oncol. 2013
Jan 22. [Epub ahead
of print]
Pelvic lymph
nodes in
locally
advanced
rectal cancer
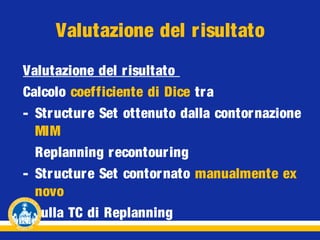
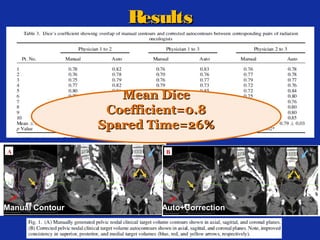
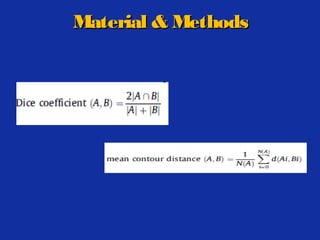
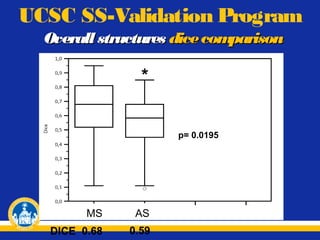
Mean Dice
coefficient
0.8
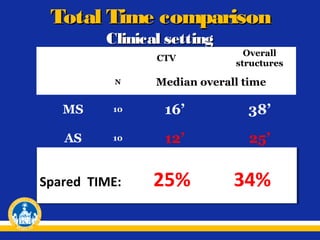
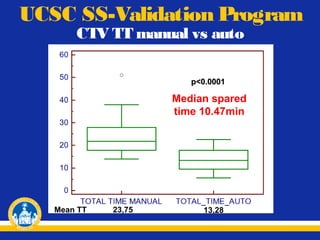
Spared
time
26%
(p<0.000001)
-
0.79-0.85
-
0.67-0.79
Sex, age, weight, height,
BMI, menopausal state,
sacro-cocciegeal
distance, most anterior
distance between upper
iliac crests
0.86-0.91
56%
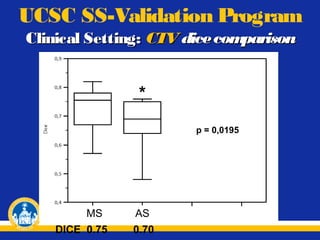
0.70
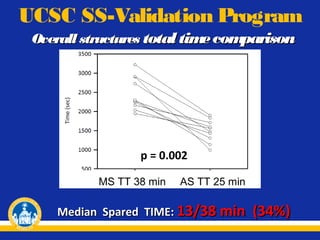
25-34%](https://image.slidesharecdn.com/dice-corso27-131015031547-phpapp01/85/Dice-corso_27-02-80-320.jpg)
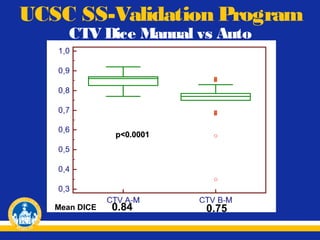

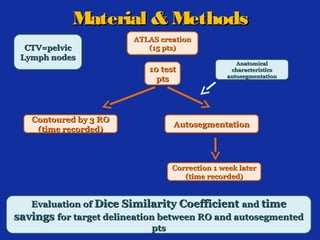
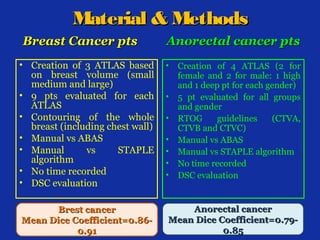
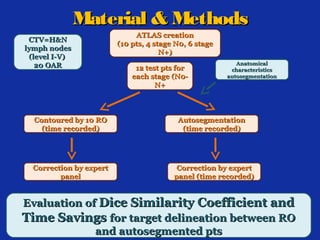
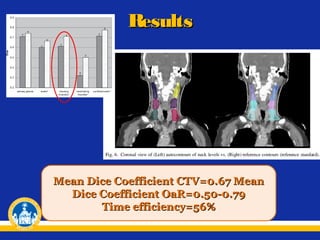
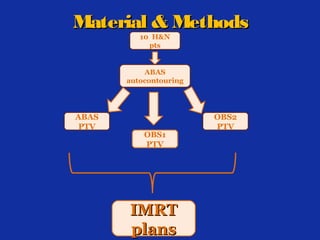
• Creation of 1 ATLAS based on 15 pts • 10 pts evaluated - Autocontours breast CTV - Autocontours breast PTV - Autocontours OARs - Autocontours pelvic lymph nodes CTV - Autocontours OARs Evaluation: Evaluation: - Dice Similarity Coefficient - Time savings - Dice Similarity Coefficient - Time savings Results Breast Cancer Anorectal Cancer Mean Dice Coefficient: Mean Dice Coefficient: CTV = 0.85 PTV = 0.80 OARs = 0.75 CTV































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)







![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)









