



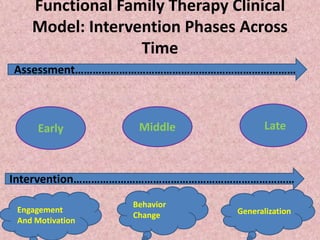
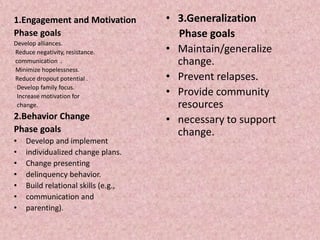
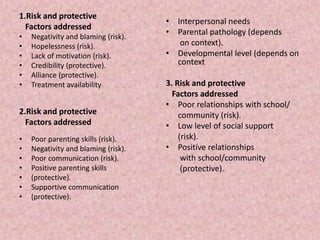

This document provides an overview of family therapy. It begins by defining family therapy as a therapeutic modality focused on interactions within a nuclear or extended family system with the goal of alleviating problems initially presented by individual members or the family as a whole. It then discusses key aspects of family therapy including that it typically involves 10-20 sessions, can be conducted in various settings, and works to change family interactions and structure. The document also summarizes different types of family therapy models including family systems therapy, structural family therapy, and functional family therapy. It provides details on functional family therapy including its goals, techniques, phases of intervention, and focus on risk and protective factors. Finally, it outlines the key concepts and goals of structural family therapy
























































![Revised Topic- Schizophrenia [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/schizophreniaautosaved-250310073514-5d1607b2-thumbnail.jpg?width=640&height=640&fit=bounds)





![Revised -ppt of child psychiatric problems [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pptofchildpsychiatricproblemsautosaved-240926091227-d0592556-thumbnail.jpg?width=640&height=640&fit=bounds)























