Downloaded 142 times


















![NVUGIH – MR5 - 12
ESGE recommends intravenous erythromycin
(single dose, 250 mg given 30 – 120 minutes prior to
upper gastrointestinal [GI] endoscopy) in patients
with clinically severe or ongoing active UGIH.
In selected patients, pre-endoscopic infusion of
erythromycin significantly improves endoscopic
visualization, reduces the need for second- look
endoscopy, decreases the number of units of
blood transfused, and reduces duration of
hospital stay.
(strong recommendation, high quality evidence).
Nonvariceal upper gastrointestinal hemorrhage: ESGE Guideline 2015](https://image.slidesharecdn.com/nvugih2015-151009083420-lva1-app6891/75/Diagnosis-and-management-of-nonvariceal-upper-gastrointestinal-hemorrhage-NVUGIH-European-Society-of-Gastrointestinal-Endoscopy-ESGE-Guideline-2015-19-2048.jpg)




























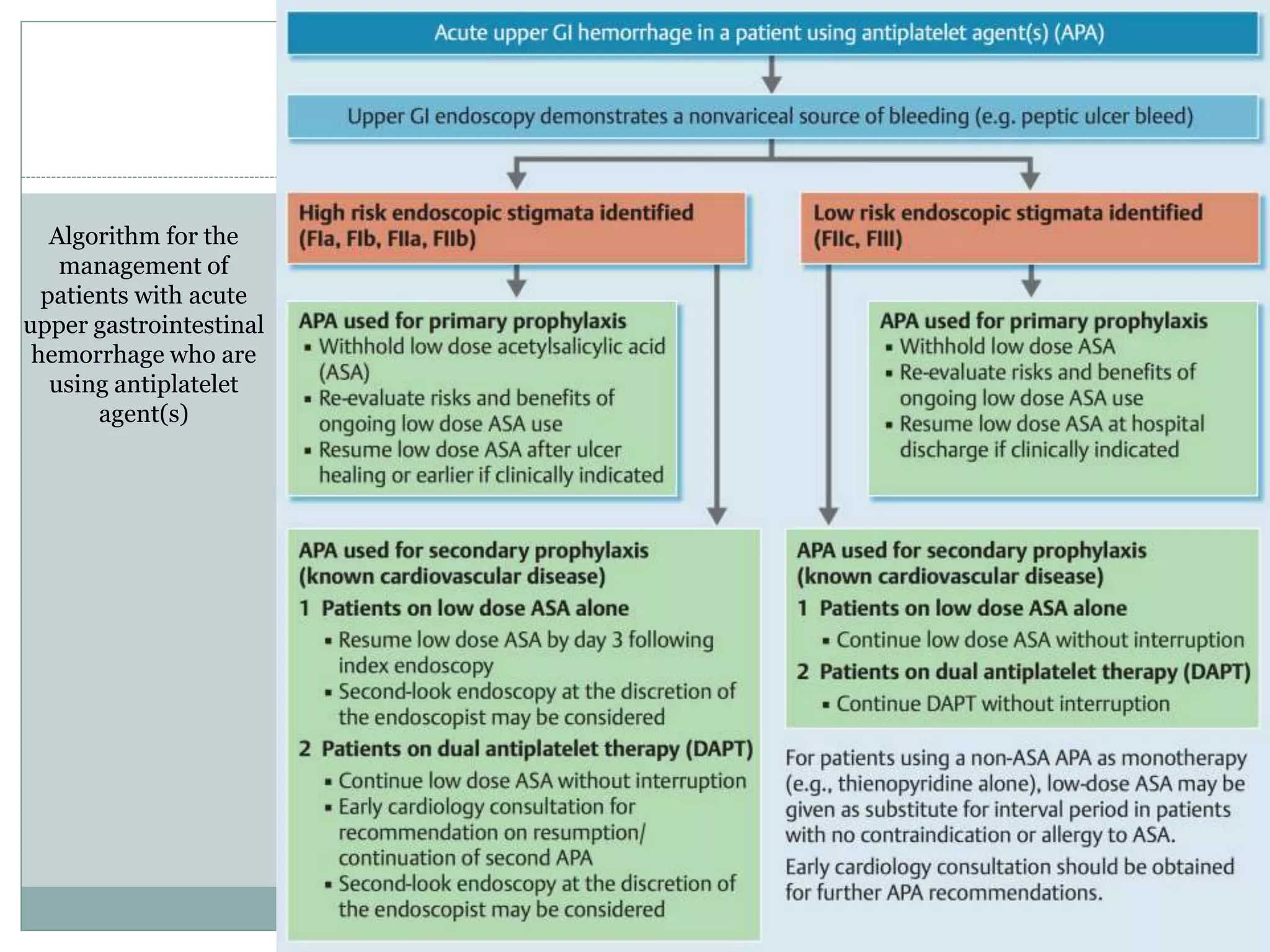




This document provides guidelines from the European Society of Gastrointestinal Endoscopy (ESGE) for the diagnosis and management of nonvariceal upper gastrointestinal hemorrhage (NVUGIH). It recommends immediate assessment of patients' hemodynamic status and volume replacement if unstable. It also recommends early upper endoscopy within 24 hours of presentation to determine the source of bleeding and apply endoscopic hemostasis as needed. The guidelines provide recommendations on risk stratification, medication management, endoscopic diagnosis and treatment options for various bleeding lesions.