Downloaded 254 times

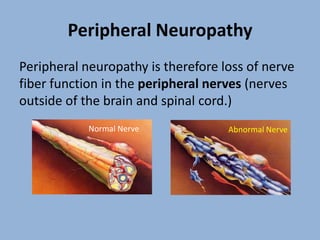






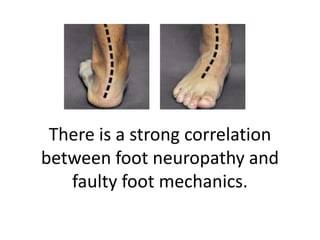

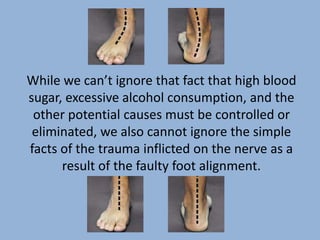



Diabetic peripheral neuropathy is a common complication of diabetes, characterized by the progressive loss of nerve function in the peripheral nerves, often leading to severe pain, foot ulcers, and amputations. Notably, the condition affects a significant percentage of diabetics, with nerve damage being exacerbated by factors such as faulty foot mechanics and long-term high blood sugar levels. The hyprocure® procedure, a minimally invasive treatment, has shown promise in alleviating nerve compression and restoring foot alignment, potentially improving outcomes for individuals suffering from this condition.











































































































