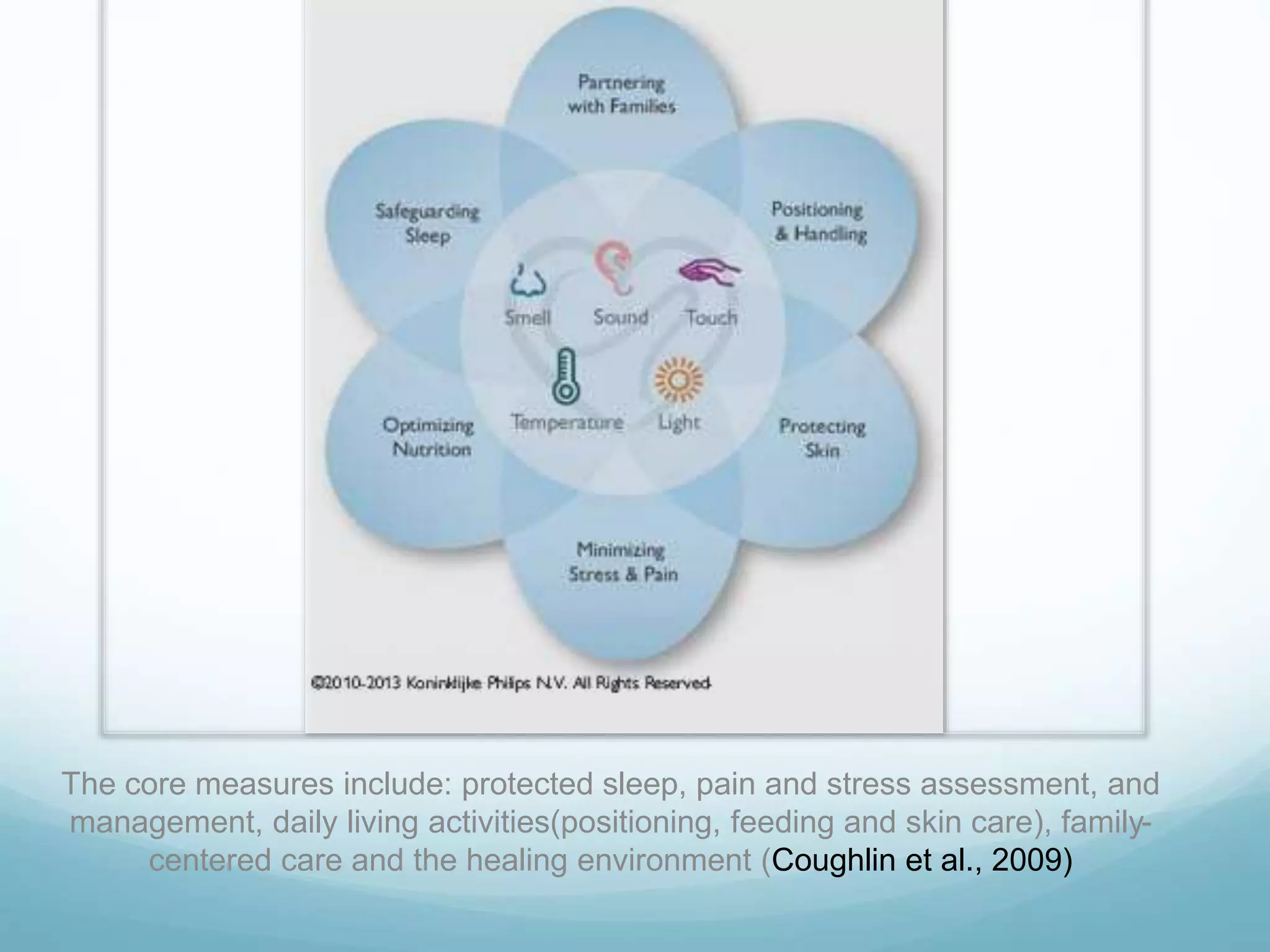
This document discusses developmental care in the NICU, which recognizes infant and family vulnerabilities and focuses on minimizing complications from hospitalization. Developmental care provides an environment that supports premature infant development through practices like cluster care, protecting sleep, and involving parents. For infants receiving respiratory support, developmental care is especially important and has been shown to lead to earlier extubation and reduced oxygen needs. Developmental care humanizes medical treatment and allows stronger emotional attachment between caregivers, parents and infants.