2. OUTLINE
•Distinguish between respiratory distress and
RDS
•Definition of RDS
•Incidence and risk factors
•Pathogenesis
•presentation
•Diagnosis
•Treatment
•Complications
•Prognosis
3. Respiratory distress is a symptom complex arising
from disease processes that cause failure to
maintain adequate gaseous exchange
•Tachypnea (>60bpm)
•Grunting, Flaring, Retractions/ recessions (GFR)
•Cynosis
•Reduced air entry
4. CAUSES OF RESPIRATORY DISTRESS
Obstruction of the airway Lung parenchymal disease
1- Choanal atresia 1- Meconium aspiration
2- Congenital stridor 2- Respiratory distress syndrome
3- Tracheal or bronchial stenosis 3- Pneumonia
4- Transient tachypnea of the newborn
(retained lung fluid)
5- Pneumothorax
6- Atelectasis
7- Congenital lobar emphysema
Non-pulmonary causes Miscellaneous
1- Heart failure 1- Disorders of the diaphragm e.g.
2- Intracranial lesions (diaphragmatic hernia)
3- Metabolic acidosis 2- Pulmonary haemorrhage
3- Pulmonary hypoplasia
5. DOWNE’s SCORING OF RESPIRATORY DISTRESS
0 1 2
Cyanosis None In room air In 40% FIO2
Retractions None Mild Severe
Audible with Audible without
Grunting None
stethoscope stethoscope
Air entry Clear Decreased or delayed Barely audible
Respiratory
Under 60 60-80 Over 80 or apnea
rate
Score:
> 4 = Clinical respiratory distress; monitor arterial blood gases
> 8 = Impending respiratory failure
6. •(RDS) is a condition of increasing respiratory
distress, commencing at, or shortly after, birth and
increasing in severity until progressive resolution
occurs among the survivors, usually around 2nd to
7th day
•Maybe primary or secondary
•Incidence and severity is inversely proportional to
gestational age
•<28wks- 60-80%
•28-32wks- 25-50%
•32-36wks- 15-30%
•>37 wks- 5%
•rare at term
7. RISK FACTORS
•Neonates younger than 33-38 weeks
•Weight less than 2500g
•Maternal diabetes
•Cesarean delivery without preceding labor
•Precipitous labor
•Fetal asphyxia
•Second of twins
•Cold stress
•Previous history of RDS in sibling
•Males
•whites
8. DECREASED RISK
•Use of antenatal steroids
•Pregnancy-induced or chronic maternal
hypertension
•Prolonged rupture of membranes
•Maternal narcotic addiction
•Chronic intrauterine stress
•IUGR or SGA
•Thyroid hormones
•Tocolytic agents
9.
10. ETIOLOGY AND PATHOPHYSIOLOGY.
• Surfactant deficiency is the 1O cause of RDS.
• Low levels of surfactant cause high surface tension
• High surface tension makes it hard to expand the
alveoli.
• Tendency of affected lungs to become atelectatic at
end-expiration when alveolar pressures are too low to
maintain alveoli in expansion
• Leads to failure to attain an adequate lung inflation
and therefore reduced gaseous exchange
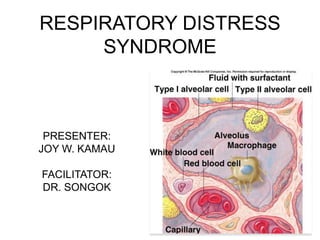
12. Structure of lung surfactant
major constituents of surfactant are dipalmitoyl phosphatidylcholine (lecithin),
phosphatidylglycerol, apoproteins (surfactant proteins SP-A, -B, -C, -D), cholesterol
13. • With advancing gestational age, increasing
amounts of phospholipids are synthesized and
stored in type II alveolar cells .
• Wk 20: start of surfactant production and storage.
Does not reach lung surface until later
• Wk 28-32: maximal production of surfactant and
appears in amniotic fluid
• Wk 34-35; mature levels of surfactant in lungs
• The amounts produced or released may be
insufficient to meet postnatal demands because of
immaturity.
• Surfactant inactivating states eg maternal DM may
lead to surfactant of lower quality/ immature
14. • Rare genetic disorders may cause fatal
respiratory distress syndrome eg.
• Abnormalities in surfactant protein B and C
genes
• gene responsible for transporting surfactant
across membranes (ABC transporter 3
[ABCA3]) are associated with severe and
often lethal familial respiratory disease
15. Prematurity, BA, hypoxemia, hypotension,
iatrogenic lung injury, cold stress
Low surfactant, high ST
Hyaline Proteinaceous Small alveolar
Difficulty
membrane outflow & units
expanding
edema
alveoli with
increased
recoil
atelectasis
Decreased
lung
compliance
16. atelectasis Decreased lung
Chest wall:
compliance
•Hyper- compliant
•Indrawing
•Low resistance to
V-Q mismatch lung recoil
Greater work of breathing
Pulmonary
vasoconstriction
Exhaustion
High P.V. resistance
apnoea
Right- left shunt
More hypoxia, worsening lung
injury
Hypercapnia, acidosis
17. pathology
Inflammation so accumulation of neutrophils in the lung
Atelectasis and hyaline membrane
Decrease fluid absorption and lung edema; liver-like lung
Hemorraghe & interstitial emhysema esp if ventilated
18. CLINICAL COURSE
• Signs of RDS in minutes to hours after birth
• Tachypnea, prominent (often audible) Grunting,
Flaring, Retractions, (GFR) and Cyanosis relatively
unresponsive to oxygen
• Breath sounds normal or harsh bronchial
• Crepitations esp over posterior lung bases
• Natural course is worsening cyanosis and dyspnea
19. • If inadequately treated, hypotension, fatigue,
cyanosis, and pallor increase
• grunting decreases or disappears as the
condition worsens
• Apnea as infants tire: OMINOUS needs
immediate intervention
• mixed respiratory-metabolic acidosis, edema,
ileus, and oliguria (end-organ damage and
complications)
20. • Respiratory failure may occur
• Usually illness peaks in 3 days, then gradual
improvement
• Improvement is often heralded by spontaneous
diuresis and the ability to oxygenate the infant at
lower inspired oxygen levels or lower ventilator
pressures
• Death may occur esp from day2-3
21. MORTALITY
• Death is rare on the 1st day,
• usually occurs between days 2 and 7
• causes are:
– alveolar air leaks (interstitial emphysema,
pneumothorax),
– pulmonary hemorrhage
– Intracranial hemorrhage
• Late mortality from bronchopulmonary
dysplasia
22. Is a Clinical diagnosis: respiratory distress occurring soon after birth.
Pay attention to risk factors! Pulse Oximetry: aim for SPO2 >85%.
ROUTINE!
Full blood count and Cultures to check for sepsis: rem culture only
positive 40-50% of the time!! gastic aspirates/ buffy smears for GBS
Chest radiograph: air bronchogram, reticular/ ground-glass appearance
after 6-12 hrs to full opacity later on.
Blood gases: hypoxia, hypercapnia, acidosis. Signs of RESP FAILURE
determine mgmt eg CPAP vs ventilation etc
Electrolytes, glucose, renal and liver function
Echocardiogram: diagnosing PDA, determine the direction and degree
of shunting, making the diagnosis of pulmonary hypertension and
excluding structural cyanotic heart disease
23.
24. Treatment of RDS
Supportive mgmt:
Oxygen at the minimum FiO2 to maintain arterial O2 at 60-
80mmhg equivalent to 85-95% SPO2.
Thermoregulation: baby in humidified (60-80%)incubator. Aim
for core temp of 36.50 C
IVF (10% dextrose; avoid fluid overload so dont go above
140ml/kg!)
Adequate caloric intake
Broad spectrum antibiotics in all infants with RDS after taking
samples for septic screen (Xpen-Genta)
Correct electrolyte imbalances
Prevent and correct anemia
May need NaHCo3 in severe acidosis (3-5mEq but based on pH
ie the lower the ph, the higher the dose)
Vitamin A 5,000 IU 3times/ wk for 4wks; reduces BPD
Endotracheal Surfactant (100mg/kg)
25. Surfactant Laboratory Container Concentration Recommended dose
Curosurf Farmalab-Chiesi 1.5 & 3 ml 80 mg/ml 100 to 200 mg/kg
Porcine
Survanta Abbott 4ml & 8 ml 25 mg/ml 100 mg/kg
Bovine
Alveofact Boeringer 1.2 ml 40 mg/ml 100 mg/kg
Bovine
Exosurf Wellcome 13.5 mg/ml(DPPC) 5 ml/kg
Synthetic
Prophylaxis of infants >1350g but with pulmonary immaturity
Propylaxis of infants <1350g at risk of RDS
Rescue therapy of infants with RDS
26. PREVENTION OF RDS
Avoid neonatal hypothermia
Good control of maternal Diabetes mellitus in pregnancy
Active mgmt of labour to avoid birth asphyxia
Prenatal corticosteroids 48hrs before delivery
Avoid unnecessary CS/ induction
Single dose surfactant to at risk, premature infants at birth
Prenatal assessment of fetal lung maturity
Lecithin –sphingomyelin ratio <1.5 prior to delivery suggests
prematurity. If >2.0, has PPV of 95-100%
Absence of phospatidylglycerol means immaturity: if
present, has PPV of 96-100%
Surfactant albumin ratio >0.47 has PPV of 95%
Lamellar body counts >30-40000 has PPV of 97%
28. Transient Tachypnea of the Newborn
Results from slow absorption of
lung fluid
Term born by LSCS/IDM /maternal
asthma
Mild respiratory distress
Peaks at about 36 hours of life
Resolve spontaneously
29. NEONATAL PNEUMONIA
Pneumonia & Sepsis have various manifestations
including typical signs of distress as well as
temperature instability
Common pathogen- Group B Streptococcus,
Staph aureus, Streptococcus aureus,
Streptococcus Pneumoniae,Gm neg rods
Risk factors- prolonged rupture of membranes,
prematurity,& maternal fever
CXR- bilateral infiltrates suggesting in utero
infection.
30. MECONIUM ASPIRATION SYNDROME
Incidence- 1.5- 2 % in term or post
term infants.
Meconium is locally irritative,
obstructive & medium for for
bacterial culture
Meconium aspiration causes
significant respiratory distress.
Hypoxia occurs because aspiration
occurs in utero.
CXR- Patchy atelectasis or
consolidation.
31. Apnea of prematurity
> 50% of infants <1500g require
intervention for apnea
Treatments
• Stimulation
• CPAP
• Intubation
• Medication:
Caffeine
Methylxanthines
Theophylline
Doxapram
• Oxygen