




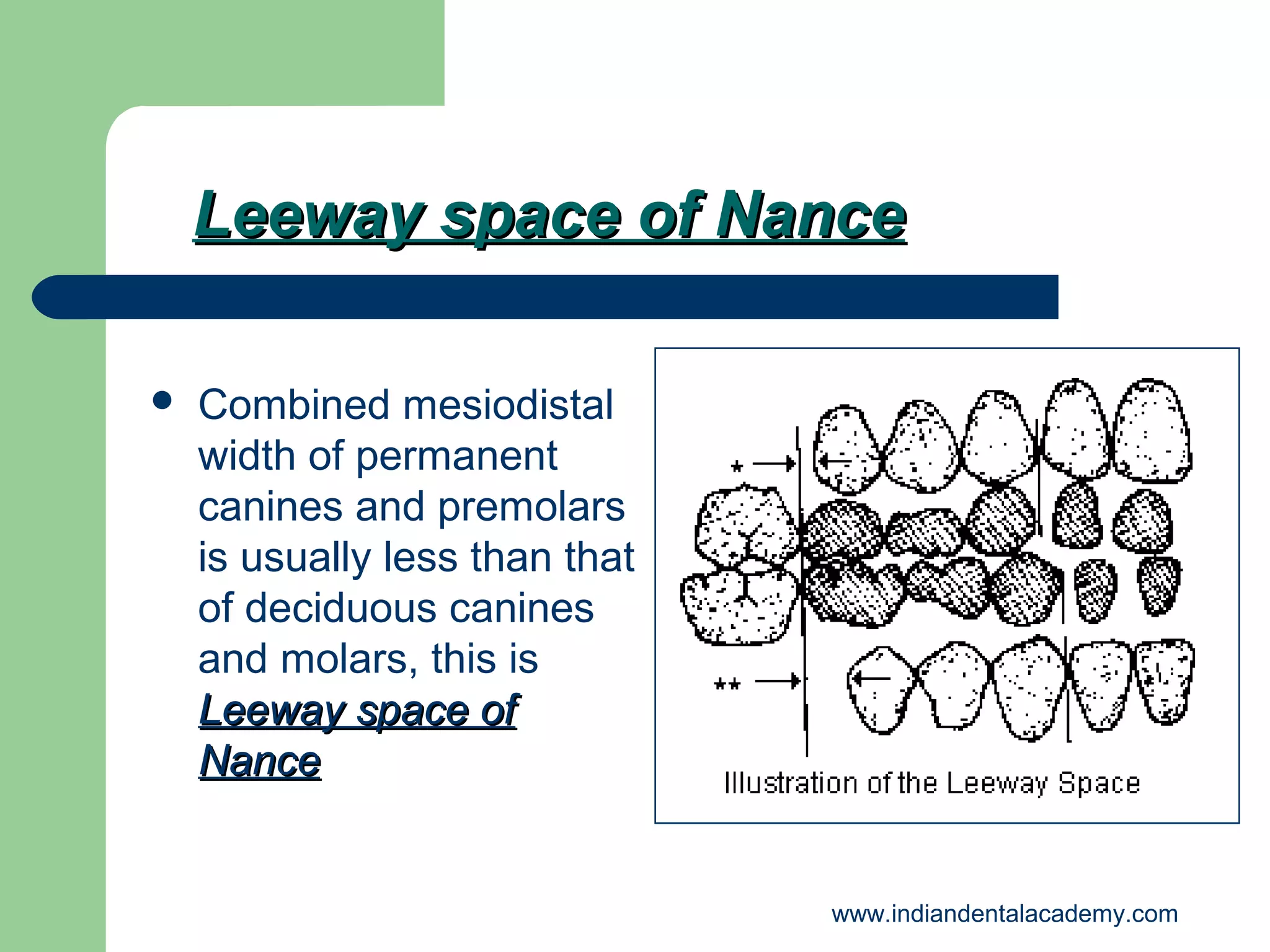
![Leeway space of Nance
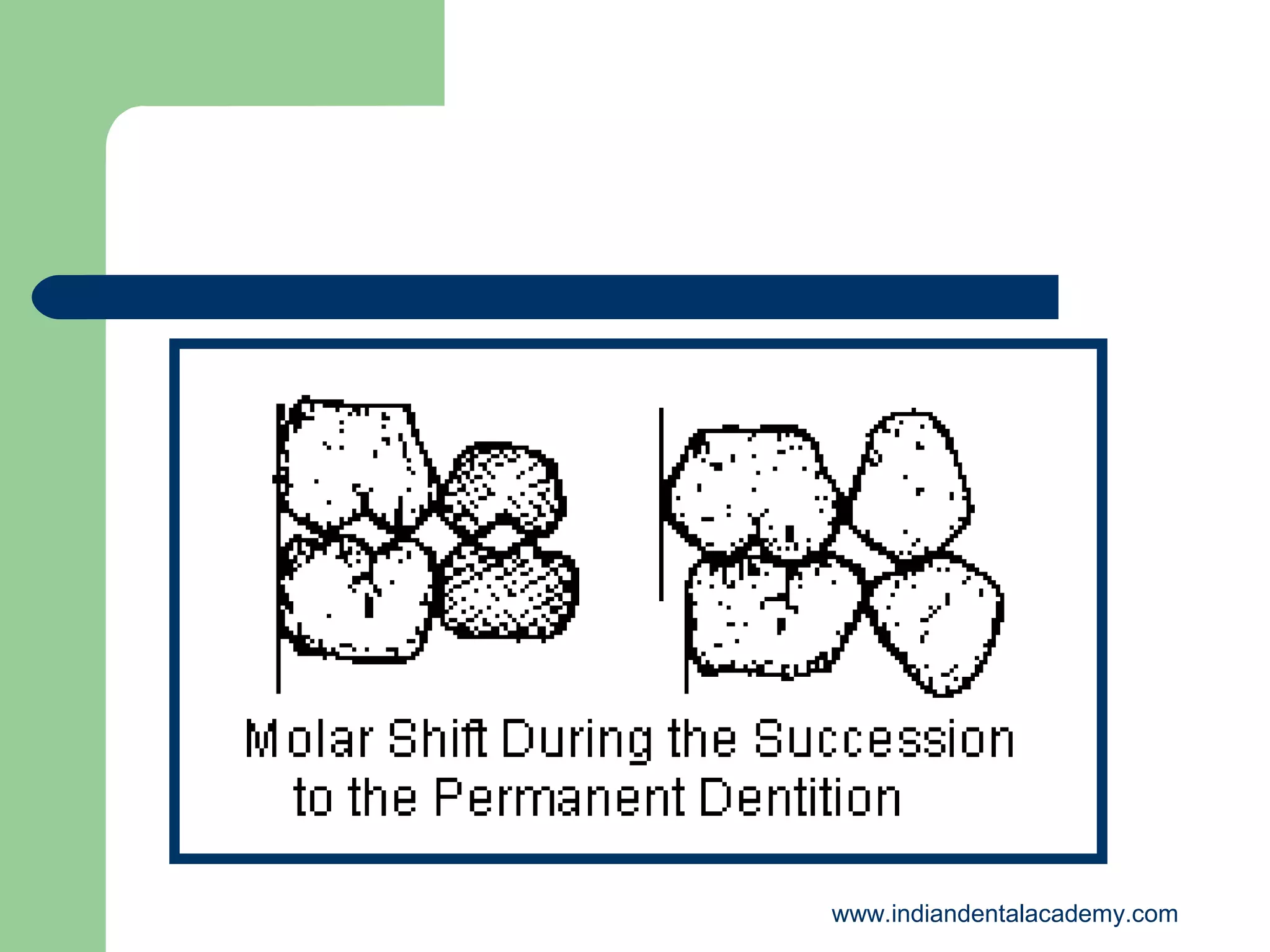
Greater in mandibular
arch [3.4mm] than in
maxillary arch [1.8mm]
This excess space is
utilized for mesial drift
of mandibular molars to
establish Class I molar
relation
www.indiandentalacademy.com](https://image.slidesharecdn.com/developmentofdentitionocclusion-131204040330-phpapp01/75/Development-of-dentition-occlusion-certified-fixed-orthodontic-courses-by-Indian-dental-academy-47-2048.jpg)

The document outlines the stages of dentition development, starting from embryonic formation to the various periods of occlusal development and eruption patterns of both deciduous and permanent teeth. Key phases include pre-dental, deciduous, mixed, and permanent dentition periods, detailing the emergence of teeth and the influence of spacing and alignment on dental health. It also discusses the physiological significance of certain dental spaces and transitions required for proper occlusion.































































































