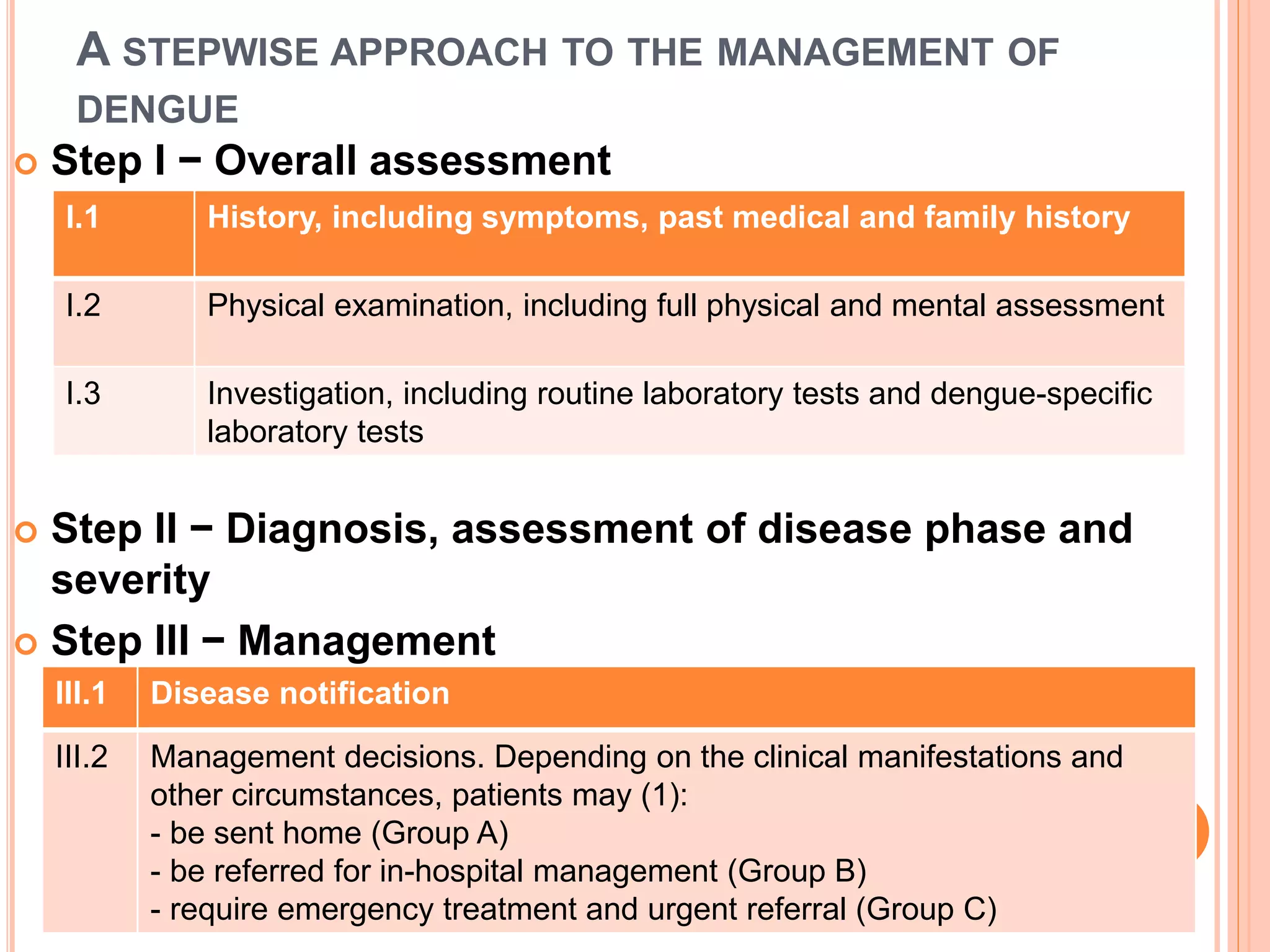
The document outlines a stepwise approach to managing dengue, including:
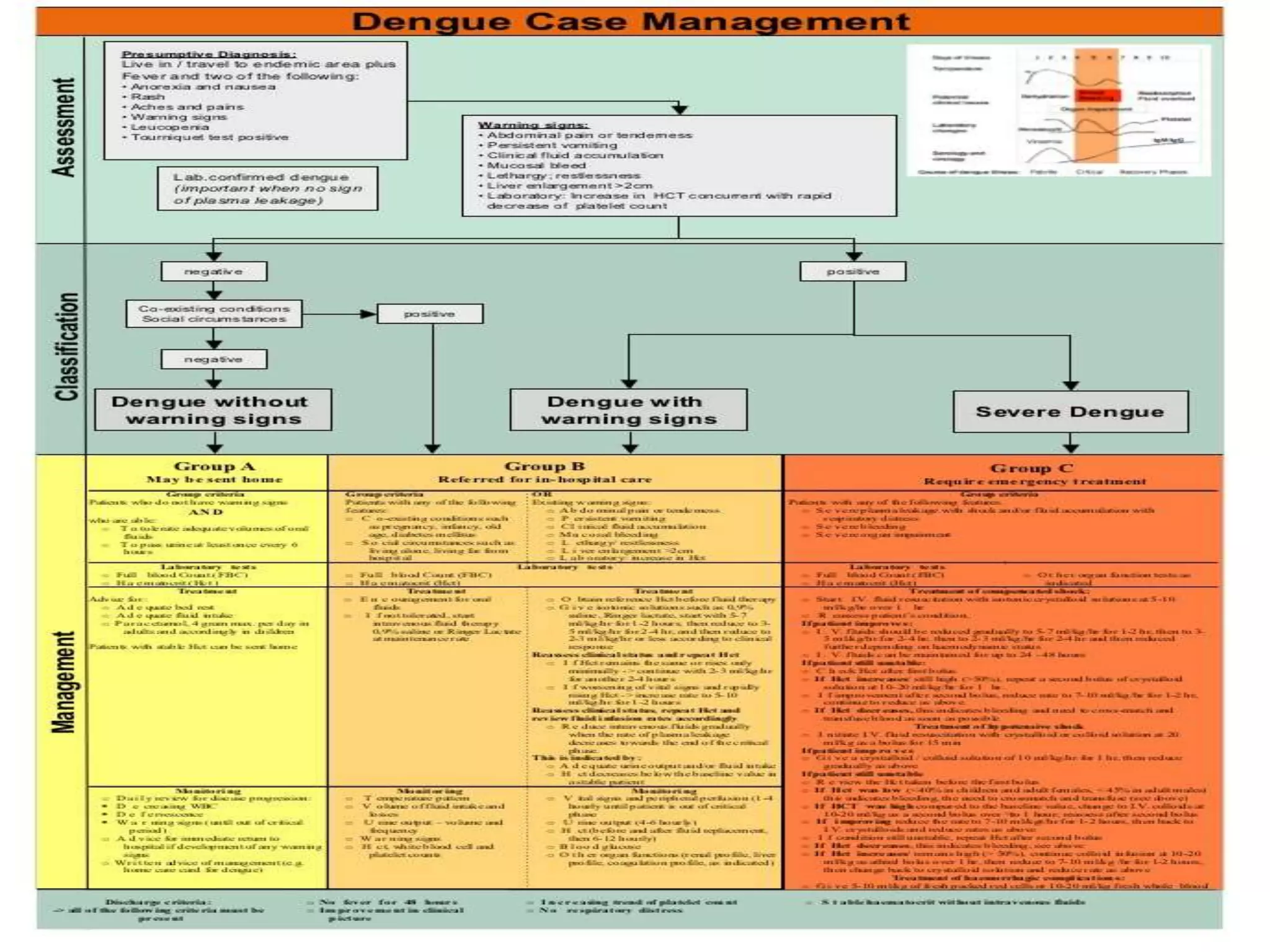
1) Assessing patients and determining if they can be sent home (Group A), require hospital admission (Group B), or emergency treatment (Group C).
2) Group A patients may be sent home with advice on rest and oral hydration if they can tolerate fluids. Group B patients require hospital admission for observation. Group C patients are in critical condition and require emergency IV fluid resuscitation.
3) Management involves close monitoring, IV fluids to correct plasma leakage, managing bleeding complications, and discharging patients once fever subsides and clinical status improves. The goal is to prevent shock through rapid fluid replacement in critical patients.